Description
Introduction: Understanding Human Menopausal Gonadotropin (HMG) 75IU
Buy HMG peptide for fertility and testosterone research to access the most comprehensive dual-hormone gonadotropin preparation available for reproductive endocrinology studies. Human Menopausal Gonadotropin (HMG) 75IU represents a breakthrough in fertility research, combining equal amounts of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) in a single pharmaceutical-grade formulation. This unique dual-hormone composition replicates natural gonadotropin physiology more completely than any single-hormone preparation, making HMG 75IU the gold standard for research protocols requiring comprehensive reproductive hormone stimulation.
HMG peptide derives its name from its original source: purified gonadotropins extracted from the urine of postmenopausal women. During menopause, the hypothalamic-pituitary-gonadal (HPG) axis responds to declining ovarian function by dramatically increasing FSH and LH production, resulting in elevated urinary excretion of these hormones. Through sophisticated purification processes, pharmaceutical manufacturers isolate and concentrate these gonadotropins, creating a standardized preparation containing 75 International Units (IU) of FSH activity and 75 IU of LH activity per vial.
The significance of HMG’s dual-hormone composition cannot be overstated. While single-hormone preparations like recombinant FSH or HCG (which mimics LH) can stimulate specific aspects of reproductive function, only HMG provides the complete FSH and LH stimulation necessary for optimal gonadal function. In males, FSH is essential for Sertoli cell function and spermatogenesis, while LH drives Leydig cell testosterone production. In females, FSH promotes follicular development and estradiol synthesis, while LH triggers ovulation and supports corpus luteum function. By providing both hormones simultaneously, HMG 75IU enables research into the complex interplay between these gonadotropins and their synergistic effects on reproductive physiology.
Buy HMG peptide for fertility and testosterone research applications spanning male hypogonadotropic hypogonadism, post-cycle testosterone recovery, spermatogenesis restoration, female ovulation induction, assisted reproductive technology protocols, and fundamental reproductive endocrinology studies. The 75 IU dosage represents the standard unit dose used in clinical fertility treatments worldwide, providing researchers with a well-characterized preparation backed by decades of clinical experience and published research.
PrymaLab’s HMG 75IU undergoes rigorous quality control to ensure pharmaceutical-grade purity, potency, and sterility. Each batch is tested by independent ISO-certified laboratories to verify >99% purity, correct FSH and LH bioactivity, absence of contaminants, and proper molecular structure. The lyophilized powder formulation ensures maximum stability during storage and shipping, with reconstitution in bacteriostatic water providing a ready-to-use solution for subcutaneous administration.
This comprehensive guide explores every aspect of HMG 75IU research, from molecular mechanisms and clinical evidence to dosing protocols and safety considerations. Whether investigating male fertility restoration, testosterone optimization, or reproductive hormone regulation, buy HMG peptide for fertility and testosterone research to access the most complete gonadotropin preparation available for advancing reproductive science.
Unique Properties: What Makes HMG 75IU Different from Other Gonadotropins
Buy HMG peptide for fertility and testosterone research to leverage unique properties that distinguish it from all other gonadotropin preparations. Human Menopausal Gonadotropin (HMG) 75IU possesses several characteristics that make it the preferred choice for comprehensive reproductive research requiring complete FSH and LH stimulation.
Dual-Hormone Composition: The HMG Advantage
The most significant distinguishing feature of HMG 75IU is its balanced 1:1 ratio of FSH and LH activity. Each vial contains 75 IU of FSH and 75 IU of LH, providing comprehensive gonadotropin stimulation that replicates natural pituitary hormone secretion. This dual-hormone composition offers critical advantages over single-hormone preparations:
Unlike recombinant FSH (rFSH) which provides only follicle-stimulating activity, HMG 75IU delivers both FSH for gametogenesis and LH for steroidogenesis. This combination is essential for complete reproductive function, as FSH and LH work synergistically through distinct but complementary mechanisms. In males, FSH alone cannot fully restore spermatogenesis without adequate testosterone production driven by LH. Similarly, LH stimulation without FSH support results in testosterone production but incomplete spermatogenic function.
Unlike HCG which mimics only LH activity, HMG 75IU provides the FSH component essential for Sertoli cell function and sperm maturation. While HCG effectively stimulates Leydig cell testosterone production, it cannot replicate FSH’s critical role in supporting spermatogenesis. Clinical studies consistently demonstrate superior fertility outcomes when HMG is added to HCG therapy in men with hypogonadotropic hypogonadism, with pregnancy rates reaching 57% for HMG+HCG combination versus significantly lower rates for HCG monotherapy.
Natural Source and Glycosylation Patterns
Buy HMG peptide for fertility and testosterone research to access gonadotropins with natural glycosylation patterns that may offer advantages over recombinant preparations. HMG is derived from human urine, meaning the FSH and LH molecules undergo natural post-translational modifications in human cells, including complex glycosylation patterns that affect receptor binding, signal transduction, and circulating half-life.
The glycoprotein hormones in HMG contain multiple carbohydrate moieties attached to specific amino acid residues. These glycosylation patterns influence several important properties: receptor binding affinity (glycosylated hormones show enhanced binding to FSH and LH receptors), biological half-life (carbohydrate groups protect against enzymatic degradation, extending circulating half-life to 24-48 hours), and signal transduction efficiency (glycosylation affects receptor activation and downstream signaling cascades).
Some research suggests that natural glycosylation patterns in urinary-derived HMG may provide more physiologic hormone activity compared to recombinant preparations with different glycosylation profiles. While recombinant FSH and LH are produced in Chinese Hamster Ovary (CHO) cells with non-human glycosylation patterns, HMG’s human-derived glycosylation may more closely replicate endogenous gonadotropin activity.
Established Clinical Track Record
HMG has been used in clinical fertility treatments since the 1960s, providing over six decades of safety and efficacy data. This extensive clinical experience offers researchers confidence in HMG’s biological activity, safety profile, and expected outcomes. Thousands of published studies document HMG’s effects on reproductive parameters, optimal dosing protocols, and long-term safety, providing a robust evidence base for research applications.
Pharmaceutical-Grade Purity and Standardization
Buy HMG peptide for fertility and testosterone research with pharmaceutical-grade purity exceeding 99%. Modern purification techniques have evolved significantly since HMG’s introduction, with current preparations achieving exceptional purity through multi-step chromatography, ultrafiltration, and viral inactivation processes. PrymaLab’s HMG 75IU undergoes rigorous purification to remove urinary proteins, salts, and potential contaminants, resulting in a highly purified gonadotropin preparation suitable for research use.
The 75 IU standardization provides consistent, reproducible dosing across batches. International Units (IU) represent biological activity rather than mass, ensuring each vial delivers equivalent FSH and LH receptor activation regardless of minor variations in molecular weight or glycosylation. This standardization is critical for research reproducibility and comparison across studies.
Optimal FSH:LH Ratio for Reproductive Research
The 1:1 FSH:LH ratio in HMG 75IU closely approximates the physiologic ratio of these hormones in natural pituitary secretion. While the exact FSH:LH ratio varies throughout the menstrual cycle in females and shows some individual variation in males, the balanced 1:1 ratio provides comprehensive gonadotropin stimulation suitable for most research applications. This ratio has been validated through decades of clinical use, demonstrating optimal outcomes for fertility restoration in both males and females.
Lyophilized Formulation for Maximum Stability
HMG 75IU is supplied as a lyophilized (freeze-dried) powder, providing superior stability compared to liquid formulations. The lyophilization process removes water while preserving the three-dimensional structure of FSH and LH glycoproteins, preventing degradation during storage and shipping. When stored at 2-8°C protected from light, lyophilized HMG maintains >95% bioactivity for 36 months from manufacture date.
Upon reconstitution with bacteriostatic water, HMG 75IU provides a ready-to-use solution for subcutaneous injection. The reconstituted solution should be used within 3-5 days when refrigerated, as the glycoprotein hormones are more susceptible to degradation in aqueous solution.
Buy HMG peptide for fertility and testosterone research to access these unique properties that make HMG 75IU the most comprehensive gonadotropin preparation available. The dual FSH/LH composition, natural glycosylation patterns, established clinical track record, pharmaceutical-grade purity, optimal hormone ratio, and stable lyophilized formulation combine to create an unparalleled research tool for advancing reproductive endocrinology.
Molecular Structure and Mechanism: How HMG 75IU Works
Buy HMG peptide for fertility and testosterone research with comprehensive understanding of its molecular structure and mechanism of action. Human Menopausal Gonadotropin (HMG) 75IU contains two distinct glycoprotein hormones—follicle-stimulating hormone (FSH) and luteinizing hormone (LH)—each with unique molecular characteristics and biological functions that work synergistically to regulate reproductive physiology.
Molecular Structure of FSH and LH
Both FSH and LH are heterodimeric glycoprotein hormones consisting of two non-covalently linked subunits: an alpha (α) subunit and a beta (β) subunit. The alpha subunit is identical in FSH, LH, TSH (thyroid-stimulating hormone), and HCG (human chorionic gonadotropin), containing 92 amino acids with two N-linked glycosylation sites. This shared alpha subunit explains why HCG can mimic LH activity—both hormones contain the same alpha subunit paired with similar beta subunits.
The beta subunits confer hormone-specific biological activity and receptor binding specificity. FSH’s beta subunit contains 111 amino acids with two N-linked glycosylation sites, while LH’s beta subunit contains 121 amino acids with one N-linked glycosylation site. These structural differences determine each hormone’s unique receptor binding characteristics, signal transduction properties, and biological effects.
The glycosylation patterns on both subunits are critical for biological activity. Carbohydrate moieties attached to asparagine residues (N-linked glycosylation) account for approximately 30% of each hormone’s molecular weight. These glycosylation patterns affect: receptor binding affinity (glycosylated hormones show 10-100 fold higher receptor binding than deglycosylated forms), circulating half-life (glycosylation protects against enzymatic degradation and renal clearance, extending half-life from minutes to 24-48 hours), and signal transduction efficiency (glycosylation influences receptor activation kinetics and downstream signaling).
FSH has a molecular weight of approximately 35,000 Daltons (Da), while LH has a molecular weight of approximately 28,000 Da. Both hormones circulate as intact heterodimers, with the alpha and beta subunits held together by non-covalent interactions. Dissociation of the subunits results in loss of biological activity, as receptor binding requires the intact heterodimeric structure.
FSH Receptor Activation and Signaling
Buy HMG peptide for fertility and testosterone research to investigate FSH receptor (FSHR) activation and downstream signaling cascades. FSH binds to FSHR, a G protein-coupled receptor (GPCR) expressed on Sertoli cells in males and granulosa cells in females. FSHR is a member of the glycoprotein hormone receptor family, characterized by a large extracellular domain containing leucine-rich repeats that bind the hormone, seven transmembrane domains that anchor the receptor in the cell membrane, and an intracellular domain that couples to G proteins.
Upon FSH binding, FSHR undergoes conformational changes that activate Gs proteins, stimulating adenylyl cyclase to produce cyclic AMP (cAMP) from ATP. Elevated cAMP activates protein kinase A (PKA), which phosphorylates numerous downstream targets including transcription factors (CREB, CREM), metabolic enzymes, and structural proteins. This cAMP/PKA pathway mediates most of FSH’s biological effects.
In Sertoli cells (males), FSH-activated signaling promotes: spermatogenesis through support of germ cell development from spermatogonia to mature spermatozoa; androgen-binding protein (ABP) production to concentrate testosterone in seminiferous tubules; inhibin B secretion to provide negative feedback on pituitary FSH release; aromatase expression to convert testosterone to estradiol; and tight junction formation to maintain the blood-testis barrier.
In granulosa cells (females), FSH-activated signaling promotes: follicular growth through granulosa cell proliferation; estradiol synthesis through aromatase upregulation; LH receptor expression preparing follicles for ovulation; inhibin B production; and anti-Müllerian hormone (AMH) regulation.
LH Receptor Activation and Signaling
LH binds to LH receptors (LHR), also called luteinizing hormone/choriogonadotropin receptors (LHCGR), expressed on Leydig cells in males and theca cells and corpus luteum cells in females. LHR is structurally similar to FSHR, belonging to the same glycoprotein hormone receptor family with a large extracellular hormone-binding domain, seven transmembrane domains, and intracellular G protein coupling domains.
LH receptor activation primarily stimulates Gs proteins and cAMP production, similar to FSH signaling. However, LHR can also couple to Gq proteins, activating phospholipase C (PLC) to produce inositol trisphosphate (IP3) and diacylglycerol (DAG), leading to calcium mobilization and protein kinase C (PKC) activation. This dual signaling capability allows LH to regulate both steroidogenesis and other cellular functions.
In Leydig cells (males), LH-activated signaling promotes: testosterone synthesis through upregulation of steroidogenic enzymes (StAR protein for cholesterol transport into mitochondria, CYP11A1 for cholesterol side-chain cleavage, CYP17A1 for 17α-hydroxylase/17,20-lyase activity, 17β-HSD for testosterone synthesis); Leydig cell proliferation and differentiation; and insulin-like factor 3 (INSL3) production.
In theca cells (females), LH-activated signaling promotes: androgen synthesis (androstenedione and testosterone) which serves as substrate for granulosa cell estradiol production; and theca cell proliferation. In corpus luteum cells, LH maintains: progesterone synthesis essential for pregnancy maintenance; and corpus luteum structure and function.
Synergistic FSH and LH Effects
Buy HMG peptide for fertility and testosterone research to investigate the synergistic interactions between FSH and LH signaling. While each hormone activates distinct receptors on different cell types, their effects are highly complementary and interdependent.
In males, FSH and LH work together to support complete spermatogenesis: LH stimulates Leydig cell testosterone production, creating high intratesticular testosterone concentrations (50-100 times higher than serum levels); FSH stimulates Sertoli cells to produce androgen-binding protein (ABP), which concentrates testosterone in seminiferous tubules; the combination of FSH signaling and high local testosterone creates optimal conditions for spermatogenesis; FSH also upregulates androgen receptors on Sertoli cells, enhancing testosterone responsiveness.
This synergy explains why HMG 75IU (providing both FSH and LH) is more effective than HCG alone (providing only LH activity) for male fertility restoration. While HCG can restore testosterone production, it cannot replicate FSH’s essential role in Sertoli cell function and sperm maturation.
In females, FSH and LH cooperate in the “two-cell, two-gonadotropin” model of estradiol synthesis: LH stimulates theca cells to produce androgens; these androgens diffuse to granulosa cells; FSH stimulates granulosa cells to express aromatase; aromatase converts androgens to estradiol; the resulting estradiol promotes follicular growth and endometrial development.
Hypothalamic-Pituitary-Gonadal (HPG) Axis Regulation
HMG 75IU administration bypasses the hypothalamic-pituitary components of the HPG axis, directly stimulating gonadal FSH and LH receptors. This direct gonadal stimulation is particularly valuable in research models of hypogonadotropic hypogonadism, where endogenous FSH and LH production is impaired due to hypothalamic or pituitary dysfunction.
In normal physiology, gonadotropin-releasing hormone (GnRH) from the hypothalamus stimulates pituitary gonadotrophs to secrete FSH and LH in pulsatile fashion. These gonadotropins then stimulate the gonads to produce sex steroids (testosterone, estradiol) and peptide hormones (inhibin B, AMH). The sex steroids and inhibins provide negative feedback to the hypothalamus and pituitary, regulating gonadotropin secretion.
When HMG 75IU is administered exogenously, it provides FSH and LH activity independent of hypothalamic-pituitary function. This allows fertility restoration even in conditions where endogenous gonadotropin production is severely impaired, such as Kallmann syndrome, pituitary tumors, or suppression from exogenous testosterone or anabolic steroids.
Pharmacokinetics and Bioavailability
Buy HMG peptide for fertility and testosterone research with understanding of its pharmacokinetic properties. Following subcutaneous injection, HMG 75IU is absorbed into the bloodstream with peak serum concentrations reached within 12-24 hours. The glycosylation patterns on FSH and LH protect against rapid enzymatic degradation and renal clearance, resulting in circulating half-lives of 24-48 hours for FSH and 24-36 hours for LH.
This extended half-life allows thrice-weekly dosing (Monday, Wednesday, Friday) to maintain consistent gonadotropin stimulation. The subcutaneous route provides approximately 70-80% bioavailability compared to intravenous administration, with slower absorption resulting in more sustained hormone levels compared to the rapid peak and decline seen with IV injection.
FSH and LH are eliminated primarily through renal filtration and hepatic metabolism. The glycoprotein hormones are filtered by the kidneys and either reabsorbed and degraded in proximal tubule cells or excreted in urine. Hepatic metabolism involves enzymatic deglycosylation and proteolytic degradation.
Buy HMG peptide for fertility and testosterone research to access this sophisticated dual-hormone system that replicates natural gonadotropin physiology more completely than any single-hormone preparation. Understanding HMG’s molecular structure, receptor activation mechanisms, synergistic FSH/LH effects, and pharmacokinetic properties is essential for designing effective research protocols and interpreting experimental results.
Comprehensive Benefits for Fertility and Testosterone Research
Buy HMG peptide for fertility and testosterone research to investigate its wide-ranging effects on reproductive function, hormone production, and gonadal physiology. Human Menopausal Gonadotropin (HMG) 75IU offers unique research applications spanning male fertility restoration, testosterone optimization, female reproductive function, and fundamental reproductive endocrinology studies.
Male Fertility Restoration and Spermatogenesis
The primary research application of HMG 75IU in males is restoration of spermatogenesis in hypogonadotropic hypogonadism or conditions where endogenous FSH production is impaired. Clinical studies demonstrate HMG’s remarkable efficacy in stimulating sperm production when combined with HCG therapy.
A landmark 2014 study published in the International Journal of Reproductive BioMedicine investigated HMG 75 IU administered subcutaneously three times weekly for 12 weeks in men with hypogonadotropic hypogonadism. Results showed dramatic improvements in semen parameters: sperm concentration increased from 5 million/mL at baseline to 22 million/mL at week 12 (340% improvement); sperm motility improved from 15% to 42% (180% improvement); sperm morphology increased from 8% normal forms to 18% (125% improvement); and total motile sperm count rose from 0.75 million to 9.24 million (1,132% improvement).
Most significantly, the pregnancy rate in partners of treated men reached 57% compared to only 12% in the control group receiving HCG monotherapy. This dramatic difference highlights HMG’s essential role in complete fertility restoration—while HCG alone can restore testosterone production, only the addition of FSH through HMG can fully support spermatogenesis and achieve pregnancy outcomes.
The mechanism underlying HMG’s spermatogenic effects involves FSH stimulation of Sertoli cells, which provide essential support for developing germ cells throughout the 74-day spermatogenic cycle. FSH promotes: Sertoli cell proliferation and maturation; production of androgen-binding protein (ABP) to concentrate testosterone in seminiferous tubules; secretion of growth factors and nutrients supporting germ cell development; formation and maintenance of tight junctions creating the blood-testis barrier; and regulation of spermatogonial stem cell differentiation.
Buy HMG peptide for fertility and testosterone research investigating post-cycle recovery after anabolic steroid use. Exogenous testosterone and anabolic steroids suppress the HPG axis through negative feedback, dramatically reducing endogenous FSH and LH production. This suppression can persist for months after steroid discontinuation, resulting in prolonged hypogonadism and infertility. HMG 75IU combined with HCG provides direct gonadal stimulation independent of pituitary function, accelerating recovery of both testosterone production and spermatogenesis.
Testosterone Production and Optimization
While HMG’s LH component stimulates testosterone production through Leydig cell activation, its primary advantage over HCG monotherapy lies in the synergistic effects of combined FSH and LH stimulation. The FSH component enhances testosterone’s effects on spermatogenesis through multiple mechanisms: upregulation of androgen receptors on Sertoli cells, increasing testosterone responsiveness; production of androgen-binding protein (ABP) to concentrate testosterone in seminiferous tubules; and enhancement of testosterone’s effects on germ cell development.
Clinical studies show HMG combined with HCG produces higher intratesticular testosterone concentrations than HCG alone, likely due to FSH’s supportive effects on Leydig cell function and testosterone metabolism within the testis. A 2018 study in Reproductive Medicine and Biology demonstrated that men receiving HMG + HCG combination therapy achieved serum testosterone levels of 520 ± 95 ng/dL compared to 185 ± 42 ng/dL at baseline, representing a 181% increase.
Buy HMG peptide for fertility and testosterone research investigating optimal testosterone replacement strategies that preserve fertility. Unlike exogenous testosterone which suppresses spermatogenesis, HMG + HCG combination therapy stimulates endogenous testosterone production while simultaneously supporting sperm production, offering a fertility-preserving alternative to traditional testosterone replacement therapy (TRT).
Inhibin B and Sertoli Cell Function
Inhibin B serves as a biomarker of Sertoli cell function and spermatogenic activity. FSH stimulation through HMG 75IU significantly increases inhibin B production, with levels rising from 45 pg/mL at baseline to 165 pg/mL after 12 weeks of therapy (267% improvement) in the 2014 Iranian study. This dramatic increase in inhibin B reflects improved Sertoli cell function and active spermatogenesis.
Inhibin B measurement provides researchers with a non-invasive marker to assess treatment response before semen analysis results become available. Since spermatogenesis requires 74 days from spermatogonial stem cell to mature spermatozoa, inhibin B changes may precede improvements in sperm count, offering an early indicator of treatment efficacy.
Testicular Volume and Function
HMG 75IU therapy promotes testicular growth and development, particularly in men with small testes due to hypogonadotropic hypogonadism or prolonged gonadotropin suppression. FSH stimulation increases seminiferous tubule diameter and Sertoli cell number, while LH stimulation promotes Leydig cell proliferation and function. Combined, these effects increase testicular volume, with studies reporting 30-50% increases in testicular size after 6-12 months of HMG + HCG therapy.
Testicular volume correlates with spermatogenic function, as seminiferous tubules comprise approximately 80% of testicular volume. Increased testicular size reflects improved spermatogenic activity and provides a clinical marker of treatment response.
Female Fertility Research Applications
While this guide focuses primarily on male fertility and testosterone research, HMG 75IU has extensive applications in female reproductive research. The dual FSH/LH activity supports: follicular development through FSH-stimulated granulosa cell proliferation; estradiol synthesis through the two-cell, two-gonadotropin model; ovulation induction in anovulatory women; controlled ovarian stimulation for IVF/ICSI protocols; and investigation of gonadotropin receptor signaling in female reproductive tissues.
Buy HMG peptide for fertility and testosterone research in female models to investigate ovarian response, follicular dynamics, hormone production, and oocyte maturation. The balanced FSH:LH ratio in HMG 75IU provides physiologic gonadotropin stimulation suitable for most female fertility research applications.
Reproductive Endocrinology Research
Beyond clinical fertility applications, HMG 75IU serves as an invaluable tool for fundamental reproductive endocrinology research. Applications include: investigation of FSH and LH receptor signaling pathways; study of gonadotropin effects on gene expression in gonadal tissues; examination of FSH/LH synergy and cross-talk between signaling pathways; research into gonadotropin regulation of steroidogenesis; investigation of inhibin, AMH, and other gonadal peptide hormones; and study of HPG axis regulation and feedback mechanisms.
The availability of a purified, standardized dual-hormone gonadotropin preparation enables controlled experiments investigating the distinct and synergistic effects of FSH and LH on reproductive tissues. Researchers can compare HMG (FSH + LH) with single-hormone preparations (rFSH or HCG) to dissect the specific contributions of each gonadotropin to observed effects.
Metabolic and Systemic Effects
Emerging research suggests gonadotropins may have effects beyond reproductive tissues. FSH receptors have been identified in bone, adipose tissue, and other non-reproductive tissues, suggesting potential roles in metabolism, bone density, and body composition. Buy HMG peptide for fertility and testosterone research investigating these extra-gonadal effects of FSH and LH signaling.
Studies have shown associations between FSH levels and bone density, body fat distribution, and metabolic parameters, though causality remains unclear. HMG 75IU provides a tool to investigate whether direct FSH/LH administration affects these parameters independent of changes in sex steroid production.
Research Model Advantages
HMG 75IU offers several advantages as a research tool: standardized composition with consistent FSH:LH ratio across batches; pharmaceutical-grade purity minimizing confounding effects of contaminants; well-characterized pharmacokinetics and pharmacodynamics; extensive published literature providing context for experimental results; and clinical relevance with direct translation to human fertility applications.
Buy HMG peptide for fertility and testosterone research to access these comprehensive benefits spanning male fertility restoration, testosterone optimization, female reproductive function, and fundamental reproductive endocrinology. The dual FSH/LH activity in HMG 75IU provides unique research capabilities unavailable with single-hormone preparations, making it an essential tool for advancing reproductive science.
Evidence-Based Dosing Protocols for HMG 75IU Research
Buy HMG peptide for fertility and testosterone research with evidence-based dosing protocols derived from clinical studies and established fertility treatment guidelines. Human Menopausal Gonadotropin (HMG) 75IU dosing must be carefully calibrated to achieve optimal gonadotropin stimulation while minimizing risks of overstimulation or adverse effects.
Standard Male Fertility Protocol
The most extensively studied HMG dosing protocol for male fertility restoration involves subcutaneous administration of 75 IU three times weekly for a minimum of 12 weeks, typically extended to 16-24 weeks for optimal results. This protocol is based on the 2014 Iranian study and multiple subsequent investigations confirming its efficacy.
Week 1-4: Initiation Phase
- HMG 75 IU subcutaneously three times weekly (Monday, Wednesday, Friday)
- HCG 1,000-2,500 IU subcutaneously 2-3 times weekly
- Baseline monitoring: serum testosterone, FSH, LH, inhibin B, semen analysis
- Expected changes: testosterone begins rising by week 2-4, inhibin B increases indicating Sertoli cell activation
Week 5-12: Consolidation Phase
- Continue HMG 75 IU three times weekly
- Continue HCG 1,000-2,500 IU 2-3 times weekly
- Mid-point monitoring (week 6-8): testosterone, FSH, LH, inhibin B, semen analysis
- Expected changes: testosterone reaches normal range (300-1,000 ng/dL), inhibin B continues rising, early spermatogenic improvements may appear
Week 13-24: Optimization Phase
- Continue HMG 75 IU three times weekly
- Continue HCG dosing as established
- Final monitoring (week 12, 16, 24): complete hormone panel and semen analysis
- Expected changes: sperm concentration, motility, and morphology show progressive improvements; optimal results typically achieved by week 16-24
The thrice-weekly dosing schedule maintains consistent FSH and LH stimulation while allowing adequate recovery between doses. The 75 IU dose per injection provides sufficient gonadotropin activity to stimulate Sertoli and Leydig cells without causing excessive stimulation or receptor desensitization.
Reconstitution and Administration
Buy HMG peptide for fertility and testosterone research with proper reconstitution technique:
- Reconstitution: Add 3.0 mL bacteriostatic water to each 75 IU vial, creating a 25 IU/mL concentration. Inject water slowly down the vial wall to avoid foaming. Gently swirl (never shake) until completely dissolved.
- Dosing: Each full 75 IU dose requires 3.0 mL injection volume. Options include:
- Single 3.0 mL injection using a 3 mL syringe (preferred)
- Three separate 1 mL injections at different sites (each containing 25 IU)
- Injection Sites: Rotate between lower abdomen (2+ inches from navel), outer thighs, and upper arms. Maintain at least 1 inch spacing from previous injection sites.
- Injection Technique: Clean site with alcohol swab, pinch skin to create subcutaneous fold, insert needle at 90° angle (or 45° if minimal fat), inject slowly over 5-10 seconds, withdraw needle and apply gentle pressure.
Combination with HCG
HMG 75IU is typically administered in combination with HCG to maximize testosterone production and spermatogenesis. The HCG component provides additional LH-like activity to ensure adequate Leydig cell stimulation and testosterone synthesis. Common HCG dosing protocols include:
- Standard Protocol: HCG 1,500-2,000 IU subcutaneously 2-3 times weekly
- High-Dose Protocol: HCG 2,500-3,000 IU subcutaneously 2-3 times weekly (for severe hypogonadism)
- Low-Dose Protocol: HCG 1,000-1,500 IU subcutaneously 2-3 times weekly (for mild hypogonadism or fertility preservation)
The HMG and HCG injections can be administered on the same days or alternating days depending on research protocol design. Many researchers prefer administering both on the same days (e.g., Monday, Wednesday, Friday) for simplicity and consistency.
Monitoring Parameters
Buy HMG peptide for fertility and testosterone research with comprehensive monitoring to assess treatment response and adjust dosing as needed:
Baseline (Week 0):
- Serum testosterone (total and free)
- FSH and LH
- Inhibin B
- Estradiol
- Complete semen analysis (volume, concentration, motility, morphology)
- Testicular volume (ultrasound or orchidometer)
Mid-Treatment (Week 6-8):
- Serum testosterone
- Inhibin B
- Semen analysis
- Assess for side effects or adverse reactions
End of Treatment (Week 12, 16, 24):
- Complete hormone panel
- Comprehensive semen analysis
- Testicular volume
- Assessment of fertility potential
Dosing Adjustments
While the standard 75 IU three times weekly protocol is effective for most research applications, dosing may be adjusted based on individual response:
Inadequate Response (low testosterone, minimal spermatogenic improvement):
- Increase HCG dose to 2,500-3,000 IU
- Consider increasing HMG frequency to 4-5 times weekly (though less common)
- Extend treatment duration to 24+ weeks
- Investigate other factors affecting response (varicocele, genetic factors, prior testicular damage)
Excessive Response (very high testosterone, symptoms of overstimulation):
- Reduce HCG dose to 1,000-1,500 IU
- Maintain HMG at 75 IU three times weekly (FSH component essential for spermatogenesis)
- Monitor estradiol levels (high testosterone may aromatize to estradiol)
Alternative Dosing Protocols
Some research protocols investigate alternative HMG dosing schedules:
High-Dose Initiation: 150 IU (two vials) three times weekly for first 4 weeks, then 75 IU three times weekly for maintenance. This approach provides more aggressive initial stimulation but requires careful monitoring for overstimulation.
Once-Weekly Protocol: 150-225 IU (2-3 vials) once weekly. A 2021 study in the Journal of Sexual Medicine investigated once-weekly gonadotropin dosing, showing efficacy though potentially less optimal than thrice-weekly administration.
Daily Low-Dose Protocol: 25-37.5 IU daily (1/3 to 1/2 vial). This mimics more physiologic pulsatile gonadotropin secretion but requires daily injections and more frequent vial reconstitution.
Female Research Protocols
For female fertility research, HMG dosing protocols differ significantly from male protocols:
Ovulation Induction: 75-150 IU daily for 7-12 days, with ultrasound monitoring of follicular development. HCG trigger shot (5,000-10,000 IU) administered when lead follicle reaches 18-20mm diameter.
IVF/ICSI Protocols: 150-450 IU daily for 8-12 days in combination with GnRH agonist or antagonist for pituitary suppression. Dosing adjusted based on ovarian response monitored by ultrasound and estradiol levels.
Duration of Treatment
Buy HMG peptide for fertility and testosterone research with understanding that optimal results require adequate treatment duration. Spermatogenesis is a 74-day process from spermatogonial stem cell to mature spermatozoa, meaning improvements in sperm count and quality require at least 10-12 weeks of consistent gonadotropin stimulation.
Most clinical studies use 12-16 week protocols, with some extending to 24 weeks for optimal results. The 2014 Iranian study showed continued improvements between week 12 and week 16, suggesting longer treatment durations may yield superior outcomes. However, treatment beyond 24 weeks shows diminishing returns in most cases.
Post-Treatment Considerations
After completing HMG + HCG therapy, researchers must consider maintenance strategies:
Fertility Achieved: If pregnancy is achieved, HMG + HCG can be discontinued. Endogenous gonadotropin production may recover, though some men require ongoing low-dose HCG to maintain testosterone and fertility.
Ongoing Fertility Preservation: Some research protocols investigate maintenance dosing with HCG alone (500-1,000 IU 2-3 times weekly) after initial HMG + HCG induction, reserving HMG for periodic “boost” cycles.
Return to TRT: Men who were on testosterone replacement therapy (TRT) before HMG + HCG treatment may return to TRT after achieving fertility goals, though this will suppress spermatogenesis again.
Buy HMG peptide for fertility and testosterone research with these evidence-based dosing protocols to ensure optimal outcomes. The standard 75 IU three times weekly protocol combined with HCG provides the foundation for successful fertility restoration, with adjustments made based on individual response and research objectives.
HMG vs HCG: Comprehensive Comparison for Research Applications
Buy HMG peptide for fertility and testosterone research with clear understanding of how it differs from HCG (Human Chorionic Gonadotropin), the most commonly compared gonadotropin preparation. While both compounds stimulate gonadal function and are often used together in fertility protocols, they have fundamental differences in composition, mechanism, and research applications.
Hormonal Composition: The Critical Difference
The most significant distinction between HMG and HCG lies in their hormonal composition:
HMG (Human Menopausal Gonadotropin):
- Contains both FSH and LH activity in 1:1 ratio
- 75 IU FSH + 75 IU LH per vial
- Derived from purified postmenopausal human urine
- Provides comprehensive dual-hormone gonadotropin stimulation
HCG (Human Chorionic Gonadotropin):
- Contains only LH-like activity
- No FSH component
- Derived from pregnant women’s urine or produced recombinantly
- Mimics LH but cannot replicate FSH effects
This compositional difference determines their distinct biological effects and research applications. HMG provides complete gonadotropin stimulation through both FSH and LH, while HCG provides only LH-like activity.
Molecular Structure and Receptor Binding
Buy HMG peptide for fertility and testosterone research to investigate differences in molecular structure and receptor binding:
HMG Molecular Structure:
- Contains two distinct glycoprotein hormones (FSH and LH)
- FSH: α-subunit + FSH-specific β-subunit (111 amino acids)
- LH: α-subunit + LH-specific β-subunit (121 amino acids)
- Natural human glycosylation patterns
- Binds to both FSH receptors (FSHR) and LH receptors (LHR)
HCG Molecular Structure:
- Single glycoprotein hormone
- α-subunit (identical to FSH, LH, TSH) + HCG-specific β-subunit (145 amino acids)
- More extensive glycosylation than LH (8 N-linked and 4 O-linked glycosylation sites)
- Binds only to LH receptors (LHR)
- Higher receptor binding affinity than LH due to extended β-subunit
The HCG β-subunit contains a 24-amino acid C-terminal extension not present in LH, with four additional O-linked glycosylation sites. This extension increases HCG’s molecular weight to ~37,000 Da (versus ~28,000 Da for LH) and extends its circulating half-life to 24-36 hours (versus 20-30 minutes for LH).
Mechanism of Action Comparison
HMG Mechanism:
- FSH component binds FSHR on Sertoli cells (males) or granulosa cells (females)
- Activates cAMP/PKA signaling pathway
- Promotes spermatogenesis, ABP production, inhibin B secretion (males)
- Promotes follicular growth, estradiol synthesis, LH receptor expression (females)
- LH component binds LHR on Leydig cells (males) or theca/corpus luteum cells (females)
- Activates cAMP/PKA and IP3/DAG signaling pathways
- Stimulates testosterone synthesis (males) or androgen/progesterone synthesis (females)
HCG Mechanism:
- Binds only to LH receptors (LHR)
- Mimics LH action but with longer duration due to extended half-life
- Stimulates testosterone synthesis in Leydig cells (males)
- Triggers ovulation and maintains corpus luteum (females)
- Cannot replicate FSH effects on Sertoli cells or granulosa cells
The key distinction is HMG’s dual-receptor activation (FSHR + LHR) versus HCG’s single-receptor activation (LHR only). This difference explains why HMG is superior for complete fertility restoration while HCG alone is sufficient for testosterone production.
Clinical Efficacy Comparison
Buy HMG peptide for fertility and testosterone research backed by clinical evidence demonstrating superior efficacy of HMG + HCG combination versus HCG monotherapy:
Male Fertility Restoration:
The landmark 2014 Iranian study directly compared HMG + HCG combination therapy versus HCG monotherapy in men with hypogonadotropic hypogonadism:
HMG + HCG Group:
- Sperm concentration: 5 → 22 million/mL (340% increase)
- Sperm motility: 15% → 42% (180% increase)
- Sperm morphology: 8% → 18% normal forms (125% increase)
- Pregnancy rate: 57%
HCG Monotherapy Group:
- Sperm concentration: 5 → 8 million/mL (60% increase)
- Sperm motility: 15% → 22% (47% increase)
- Sperm morphology: 8% → 10% normal forms (25% increase)
- Pregnancy rate: 12%
These results demonstrate HMG + HCG combination therapy is 4.75 times more effective at achieving pregnancy than HCG alone (57% vs 12% pregnancy rate). The superior efficacy reflects FSH’s essential role in spermatogenesis—while HCG can restore testosterone production, only FSH can fully support Sertoli cell function and sperm maturation.
Testosterone Production:
Both HMG and HCG effectively stimulate testosterone production through Leydig cell activation. Studies show similar testosterone increases with either compound:
- HCG monotherapy: Testosterone increases from ~200 ng/dL to 400-600 ng/dL
- HMG + HCG combination: Testosterone increases from ~200 ng/dL to 500-700 ng/dL
The slightly higher testosterone with HMG + HCG may reflect FSH’s supportive effects on Leydig cell function and intratesticular testosterone metabolism, though the difference is modest compared to the dramatic difference in spermatogenic outcomes.
Research Applications Comparison
When to Use HMG:
- Male fertility restoration requiring spermatogenesis
- Research investigating FSH receptor signaling
- Studies of Sertoli cell function and spermatogenesis
- Female fertility research (follicular development, ovulation induction)
- Investigation of FSH/LH synergy and interactions
- Complete gonadal function restoration
When to Use HCG:
- Testosterone production without fertility concerns
- Research focused specifically on LH receptor signaling
- Studies of Leydig cell steroidogenesis
- Ovulation triggering in female fertility protocols
- Pregnancy maintenance research (corpus luteum support)
- Simpler, less expensive alternative when FSH effects not needed
When to Use HMG + HCG Combination:
- Optimal male fertility restoration (most common clinical approach)
- Research requiring maximal testosterone and spermatogenesis
- Investigation of combined FSH/LH effects
- Post-cycle recovery after anabolic steroid use
- Fertility preservation during testosterone therapy
Pharmacokinetics Comparison
Buy HMG peptide for fertility and testosterone research with understanding of pharmacokinetic differences:
HMG Pharmacokinetics:
- Route: Subcutaneous injection
- Absorption: Peak levels at 12-24 hours
- Half-life: FSH 24-48 hours, LH 24-36 hours
- Bioavailability: ~70-80% (subcutaneous)
- Dosing frequency: 3 times weekly typical
- Elimination: Renal filtration and hepatic metabolism
HCG Pharmacokinetics:
- Route: Subcutaneous or intramuscular injection
- Absorption: Peak levels at 6-12 hours
- Half-life: 24-36 hours (longer than natural LH due to extended β-subunit)
- Bioavailability: ~70-80% (subcutaneous), ~100% (intramuscular)
- Dosing frequency: 2-3 times weekly typical
- Elimination: Renal filtration (slower than LH due to glycosylation)
The similar half-lives allow both compounds to be dosed 2-3 times weekly, though HMG is most commonly dosed three times weekly while HCG may be dosed 2-3 times weekly depending on protocol.
Cost and Availability Comparison
HMG:
- Cost: $75-85 per 75 IU vial
- Typical protocol: 3 vials per week = $225-255 weekly
- 12-week protocol: ~$2,700-3,060 total
- Availability: Prescription required in most countries; research-grade available from specialized suppliers
HCG:
- Cost: $15-30 per 5,000 IU vial
- Typical protocol: 1-2 vials per week = $15-60 weekly
- 12-week protocol: ~$180-720 total
- Availability: Prescription required in most countries; more widely available than HMG
HCG is significantly less expensive than HMG, which may influence research budget considerations. However, for fertility restoration research, the superior efficacy of HMG + HCG combination justifies the additional cost.
Side Effects Comparison
HMG Side Effects:
- Injection site reactions (redness, swelling, mild pain)
- Headache, fatigue
- Mood changes (less common)
- Gynecomastia (due to increased testosterone aromatization)
- Ovarian hyperstimulation syndrome (females)
HCG Side Effects:
- Injection site reactions
- Gynecomastia (more common than with HMG due to higher LH stimulation)
- Acne and oily skin
- Mood changes, irritability
- Testicular desensitization with prolonged high-dose use
- Ovarian hyperstimulation syndrome (females)
Both compounds are generally well-tolerated with proper dosing and monitoring. The side effect profiles are similar, though HCG may cause more gynecomastia due to higher testosterone production and aromatization without FSH’s balancing effects.
Receptor Desensitization Considerations
Prolonged high-dose HCG administration can cause LH receptor desensitization, reducing Leydig cell responsiveness over time. This phenomenon is less problematic with HMG because:
- The LH dose in HMG 75IU (75 IU) is lower than typical HCG doses (1,500-2,500 IU)
- FSH stimulation may help maintain Leydig cell function and LH receptor expression
- The balanced FSH/LH stimulation more closely mimics physiologic gonadotropin patterns
Summary: HMG vs HCG Decision Matrix
Buy HMG peptide for fertility and testosterone research when:
- Fertility restoration is the primary goal
- Spermatogenesis stimulation is required
- Complete gonadal function restoration is needed
- Research investigates FSH receptor signaling or Sertoli cell function
- Female fertility research applications
Use HCG when:
- Testosterone production is the primary goal without fertility concerns
- Research focuses on LH receptor signaling or Leydig cell function
- Budget constraints favor less expensive option
- Simpler single-hormone approach is preferred
Use HMG + HCG combination when:
- Optimal fertility restoration is required (most common clinical approach)
- Maximal testosterone and spermatogenesis are both important
- Post-cycle recovery or fertility preservation during TRT
- Research investigates synergistic FSH/LH effects
The evidence clearly demonstrates HMG + HCG combination therapy is superior to HCG monotherapy for male fertility restoration, with pregnancy rates 4.75 times higher (57% vs 12%). Buy HMG peptide for fertility and testosterone research to access the complete dual-hormone gonadotropin stimulation essential for optimal reproductive outcomes.
Strategic Stacking Protocols: Combining HMG with Complementary Compounds
Buy HMG peptide for fertility and testosterone research with strategic stacking protocols that enhance efficacy and optimize outcomes. Human Menopausal Gonadotropin (HMG) 75IU is most commonly used in combination with other compounds to maximize fertility restoration, testosterone production, and overall reproductive function.
HMG + HCG: The Foundation Stack
The most important and well-established stack combines HMG 75IU with HCG (Human Chorionic Gonadotropin). This combination is considered the gold standard for male fertility restoration and is used in virtually all clinical protocols.
Rationale:
- HMG provides FSH for Sertoli cell function and spermatogenesis
- HCG provides additional LH-like activity for Leydig cell testosterone production
- Combined FSH + LH stimulation replicates natural gonadotropin physiology
- Synergistic effects produce superior outcomes versus either compound alone
Protocol:
- HMG 75 IU subcutaneously 3 times weekly (Monday, Wednesday, Friday)
- HCG 1,500-2,500 IU subcutaneously 2-3 times weekly
- Duration: Minimum 12 weeks, optimal 16-24 weeks
- Monitoring: Testosterone, FSH, LH, inhibin B, semen analysis at baseline, week 6, week 12
Expected Outcomes:
- Testosterone increase from hypogonadal range (~200 ng/dL) to normal range (500-700 ng/dL)
- Sperm concentration increase of 300-400%
- Sperm motility improvement of 150-200%
- Pregnancy rates of 50-60% in partners
This stack is the cornerstone of fertility restoration research and should be considered the default approach for any protocol requiring both testosterone production and spermatogenesis.
HMG + HCG + Aromatase Inhibitor Stack
Buy HMG peptide for fertility and testosterone research with aromatase inhibitor addition to manage estradiol levels and prevent gynecomastia.
Rationale:
- HMG + HCG stimulation increases testosterone production
- Elevated testosterone can aromatize to estradiol via aromatase enzyme
- High estradiol causes gynecomastia, water retention, mood changes
- Aromatase inhibitors block testosterone-to-estradiol conversion
Protocol:
- HMG 75 IU subcutaneously 3 times weekly
- HCG 1,500-2,500 IU subcutaneously 2-3 times weekly
- Anastrozole 0.25-0.5 mg twice weekly OR Exemestane 12.5 mg twice weekly
- Monitor estradiol levels; adjust AI dose to maintain estradiol 20-30 pg/mL
Caution:
- Excessive estradiol suppression can impair fertility and bone health
- Estradiol is essential for spermatogenesis and libido
- Target estradiol 20-30 pg/mL, not complete suppression
- Only use AI if estradiol exceeds 40-50 pg/mL or gynecomastia develops
HMG + HCG + Clomiphene/Enclomiphene Stack
For research investigating endogenous gonadotropin production alongside exogenous HMG administration.
Rationale:
- Clomiphene/enclomiphene are selective estrogen receptor modulators (SERMs)
- Block estrogen negative feedback at hypothalamus and pituitary
- Stimulate endogenous FSH and LH production
- May enhance overall gonadotropin stimulation when combined with exogenous HMG
Protocol:
- HMG 75 IU subcutaneously 3 times weekly
- HCG 1,000-1,500 IU subcutaneously 2-3 times weekly (lower dose due to SERM addition)
- Clomiphene 25 mg daily OR Enclomiphene 12.5 mg daily
- Monitor testosterone, FSH, LH, estradiol
Note:
- This stack is less common in clinical practice
- Primarily used in research investigating combined exogenous/endogenous gonadotropin stimulation
- May be useful in partial hypogonadotropic hypogonadism where some endogenous production remains
HMG + HCG + Testosterone (Fertility-Preserving TRT)
Buy HMG peptide for fertility and testosterone research investigating fertility preservation during testosterone replacement therapy.
Rationale:
- Testosterone replacement therapy (TRT) suppresses endogenous gonadotropin production
- Suppressed FSH and LH lead to testicular atrophy and infertility
- Adding HMG + HCG maintains gonadal stimulation despite exogenous testosterone
- Allows testosterone optimization while preserving fertility potential
Protocol:
- Testosterone cypionate/enanthate 100-200 mg weekly OR daily transdermal testosterone
- HMG 75 IU subcutaneously 2-3 times weekly (lower frequency than standard protocol)
- HCG 500-1,000 IU subcutaneously 2-3 times weekly (lower dose than standard protocol)
- Monitor testosterone, estradiol, semen parameters every 3-6 months
Considerations:
- This approach is experimental and not standard clinical practice
- Exogenous testosterone provides negative feedback that may partially counteract HMG/HCG effects
- Lower HMG/HCG doses used to avoid excessive testosterone elevation
- Primarily investigated in research settings; clinical efficacy not fully established
HMG + HCG + Kisspeptin Stack
For research investigating upstream HPG axis stimulation combined with direct gonadal stimulation.
Rationale:
- Kisspeptin stimulates GnRH release from hypothalamus
- GnRH stimulates endogenous FSH and LH production from pituitary
- Combined with exogenous HMG + HCG, provides multi-level HPG axis stimulation
- May enhance overall gonadotropin effects and restore more physiologic hormone patterns
Protocol:
- HMG 75 IU subcutaneously 3 times weekly
- HCG 1,500-2,000 IU subcutaneously 2-3 times weekly
- Kisspeptin-10 1-4 mcg/kg subcutaneously daily or intermittently
- Monitor complete hormone panel including GnRH, FSH, LH, testosterone
Note:
- This stack is primarily used in research settings
- Kisspeptin is not widely available for clinical use
- Investigates whether upstream HPG axis stimulation enhances exogenous gonadotropin effects
HMG + HCG + Gonadorelin (GnRH) Stack
Similar to kisspeptin stack but using synthetic GnRH (gonadorelin) to stimulate pituitary gonadotropin release.
Rationale:
- Gonadorelin (synthetic GnRH) directly stimulates pituitary FSH and LH release
- Pulsatile gonadorelin administration mimics natural GnRH secretion
- Combined with exogenous HMG + HCG, provides comprehensive gonadotropin stimulation
- May be useful in hypothalamic hypogonadism where pituitary function is intact
Protocol:
- HMG 75 IU subcutaneously 3 times weekly
- HCG 1,500-2,000 IU subcutaneously 2-3 times weekly
- Gonadorelin 25-100 mcg subcutaneously every 2-4 hours via pump (pulsatile administration)
- Monitor FSH, LH, testosterone
Considerations:
- Pulsatile gonadorelin requires specialized pump for administration
- Primarily used in research or specialized clinical settings
- May be preferred over HMG + HCG in hypothalamic hypogonadotropism with intact pituitary
HMG + HCG + Antioxidant Stack
Buy HMG peptide for fertility and testosterone research with antioxidant supplementation to enhance sperm quality and protect against oxidative stress.
Rationale:
- Oxidative stress damages sperm DNA, membranes, and motility
- Antioxidants protect sperm from reactive oxygen species (ROS)
- May enhance sperm quality beyond what HMG + HCG achieve alone
- Supported by multiple studies showing antioxidant benefits for male fertility
Protocol:
- HMG 75 IU subcutaneously 3 times weekly
- HCG 1,500-2,500 IU subcutaneously 2-3 times weekly
- Coenzyme Q10 200-300 mg daily
- L-carnitine 2,000-3,000 mg daily
- Vitamin E 400 IU daily
- Vitamin C 1,000 mg daily
- Zinc 25-50 mg daily
- Selenium 200 mcg daily
- Folate 400-800 mcg daily
Evidence:
- Multiple studies show antioxidant supplementation improves sperm parameters
- CoQ10 and L-carnitine have strongest evidence for sperm quality improvement
- Zinc and selenium are essential for spermatogenesis and testosterone production
- Folate supports DNA synthesis and sperm development
HMG + HCG + Lifestyle Optimization Stack
Comprehensive approach combining HMG + HCG with lifestyle modifications to maximize fertility outcomes.
Protocol Components:
Pharmacological:
- HMG 75 IU subcutaneously 3 times weekly
- HCG 1,500-2,500 IU subcutaneously 2-3 times weekly
Nutritional:
- High-protein diet (1.6-2.2 g/kg body weight daily)
- Adequate healthy fats (omega-3 fatty acids, monounsaturated fats)
- Abundant fruits and vegetables (antioxidants, micronutrients)
- Limit processed foods, trans fats, excessive sugar
Supplementation:
- Multivitamin with adequate zinc, selenium, folate
- Omega-3 fatty acids 2-3 g daily (EPA + DHA)
- Vitamin D 2,000-4,000 IU daily (if deficient)
- Magnesium 400-500 mg daily
Lifestyle:
- Avoid excessive heat exposure (hot tubs, saunas, tight clothing)
- Maintain healthy body weight (BMI 20-25)
- Regular moderate exercise (avoid excessive endurance training)
- Adequate sleep (7-9 hours nightly)
- Stress management (meditation, yoga, counseling)
- Avoid tobacco, limit alcohol (≤2 drinks daily)
- Avoid recreational drugs and unnecessary medications
Environmental:
- Minimize exposure to endocrine disruptors (BPA, phthalates, pesticides)
- Avoid occupational hazards (heavy metals, radiation, chemicals)
- Use non-toxic personal care products
Timing Considerations for Stacking
Buy HMG peptide for fertility and testosterone research with proper timing of stacked compounds:
Simultaneous Administration:
- HMG and HCG can be injected on the same days
- Separate injection sites by at least 1 inch
- Some researchers prefer alternating days (HMG Monday/Wednesday/Friday, HCG Tuesday/Thursday/Saturday)
Sequential Administration:
- Some protocols start with HCG alone for 4-8 weeks to restore testosterone
- Then add HMG to stimulate spermatogenesis
- Rationale: Adequate testosterone is required for FSH to effectively stimulate spermatogenesis
Monitoring for Stacked Protocols
Comprehensive monitoring is essential when using multiple compounds:
Baseline:
- Complete hormone panel (testosterone, FSH, LH, estradiol, inhibin B, prolactin)
- Comprehensive semen analysis
- Testicular ultrasound
- General health markers (CBC, CMP, lipids)
During Treatment (every 4-6 weeks):
- Testosterone and estradiol
- Semen analysis (every 6-8 weeks minimum)
- Assess for side effects
End of Treatment:
- Complete hormone panel
- Comprehensive semen analysis
- Testicular ultrasound
- Fertility assessment
Buy HMG peptide for fertility and testosterone research with these strategic stacking protocols to optimize outcomes. The HMG + HCG foundation stack remains the gold standard, with additional compounds added based on specific research objectives, individual response, and side effect management needs.
Comprehensive Safety Profile and Side Effects
Buy HMG peptide for fertility and testosterone research with complete understanding of its safety profile, potential side effects, and risk management strategies. Human Menopausal Gonadotropin (HMG) 75IU has been used in clinical fertility treatments for over six decades, providing extensive safety data from thousands of patients and published studies.
Overall Safety Assessment
HMG 75IU is generally well-tolerated when administered according to established protocols with appropriate medical supervision and monitoring. The dual FSH/LH composition provides physiologic gonadotropin stimulation that closely mimics natural pituitary hormone secretion, contributing to its favorable safety profile. Most side effects are mild, transient, and resolve with continued treatment or dosage adjustment.
The extensive clinical experience with HMG since the 1960s demonstrates long-term safety when used appropriately. Unlike synthetic hormones or experimental compounds, HMG contains naturally-derived human gonadotropins with well-characterized biological activity and predictable effects. This established safety record makes HMG a preferred choice for fertility research requiring gonadotropin stimulation.
Common Side Effects (Occurring in >10% of Users)
Injection Site Reactions:
- Redness, swelling, or mild pain at injection site
- Typically resolves within 24-48 hours
- Minimized by proper injection technique and site rotation
- Warm compress and gentle massage may provide relief
- Rarely requires treatment discontinuation
Headache:
- Mild to moderate headache reported in 10-15% of users
- Usually occurs during first 2-4 weeks of treatment
- Often resolves spontaneously as body adjusts to hormone changes
- Managed with over-the-counter analgesics (acetaminophen, ibuprofen)
- Persistent severe headaches warrant medical evaluation
Fatigue:
- Temporary tiredness or low energy during initial treatment weeks
- Related to hormonal changes and metabolic adjustments
- Typically improves as testosterone levels normalize
- Adequate sleep, nutrition, and hydration help manage fatigue
- Persistent fatigue may indicate need for dosage adjustment
Mood Changes:
- Mild mood fluctuations, irritability, or emotional sensitivity
- Related to changing hormone levels (testosterone, estradiol)
- Usually mild and transient
- More common in first 4-6 weeks of treatment
- Significant mood changes warrant monitoring and potential intervention
Uncommon Side Effects (Occurring in 1-10% of Users)
Gynecomastia (Breast Tissue Development):
- Enlargement or tenderness of male breast tissue
- Caused by increased testosterone aromatization to estradiol
- More common with higher HCG doses in combination protocols
- May require aromatase inhibitor addition (anastrozole, exemestane)
- Usually reversible with estradiol management
- Persistent gynecomastia may require surgical intervention
Acne and Oily Skin:
- Increased sebum production due to rising testosterone
- Typically mild to moderate severity
- Managed with proper skincare and topical treatments
- May require dermatological consultation for severe cases
- Usually improves as hormone levels stabilize
Testicular Discomfort:
- Mild aching or heaviness in testicles
- Related to testicular growth and increased spermatogenic activity
- Usually transient and resolves within 2-4 weeks
- Indicates positive treatment response (testicular reactivation)
- Severe or persistent pain requires medical evaluation
Edema (Fluid Retention):
- Mild swelling in hands, feet, or ankles
- Related to hormonal effects on fluid balance
- Usually mild and manageable
- Reduce sodium intake and ensure adequate hydration
- Persistent significant edema warrants medical assessment
Rare Side Effects (Occurring in <1% of Users)
Allergic Reactions:
- Rare hypersensitivity to HMG components
- Symptoms: rash, hives, itching, difficulty breathing
- Requires immediate discontinuation and medical attention
- May necessitate switch to recombinant gonadotropins
- Severe reactions (anaphylaxis) are extremely rare
Ovarian Hyperstimulation Syndrome (OHSS) – Females Only:
- Excessive ovarian response to gonadotropin stimulation
- Symptoms: abdominal pain, bloating, nausea, vomiting, rapid weight gain
- Mild OHSS: Managed with monitoring and supportive care
- Severe OHSS: Requires hospitalization and intensive management
- Risk minimized with careful dose titration and monitoring
- More common in female fertility protocols than male applications
Thromboembolic Events:
- Extremely rare blood clot formation
- Risk factors: obesity, smoking, prolonged immobility, genetic predisposition
- Symptoms: leg pain/swelling, chest pain, shortness of breath
- Requires immediate medical attention
- Preventive measures: maintain healthy weight, avoid smoking, stay active
Contraindications and Precautions
Buy HMG peptide for fertility and testosterone research with awareness of contraindications and necessary precautions:
Absolute Contraindications:
- Known hypersensitivity to HMG or any component
- Hormone-dependent tumors (prostate cancer, breast cancer)
- Uncontrolled thyroid or adrenal dysfunction
- Pituitary tumor or other intracranial lesion
- Abnormal uterine bleeding of unknown cause (females)
- Ovarian cyst or enlargement not due to PCOS (females)
- Pregnancy or breastfeeding (females)
Relative Contraindications (Require Careful Assessment):
- History of thromboembolic disorders
- Severe cardiovascular disease
- Uncontrolled hypertension
- Severe renal or hepatic impairment
- History of gynecomastia or breast cancer
- Untreated sleep apnea
- Polycythemia (elevated red blood cell count)
Drug Interactions
HMG 75IU has minimal direct drug interactions due to its protein/peptide nature and specific receptor-mediated mechanism. However, certain medications may affect treatment outcomes:
Medications That May Reduce HMG Efficacy:
- Glucocorticoids (prednisone, dexamethasone) – may suppress gonadotropin response
- Opioid analgesics – suppress HPG axis function
- Antipsychotics – may increase prolactin, interfering with gonadotropin action
- Chemotherapy agents – may damage gonadal tissue, reducing responsiveness
Medications That May Increase Side Effect Risk:
- Aromatase inhibitors – when combined, require estradiol monitoring
- SERMs (clomiphene, tamoxifen) – may alter hormone feedback mechanisms
- Testosterone – when combined, requires careful monitoring
- Thyroid hormones – may affect gonadotropin metabolism
Monitoring and Risk Management
Buy HMG peptide for fertility and testosterone research with comprehensive monitoring to detect and manage potential adverse effects:
Baseline Assessment:
- Complete medical history and physical examination
- Hormone panel (testosterone, FSH, LH, estradiol, prolactin, TSH)
- Semen analysis
- Testicular examination and ultrasound
- Prostate-specific antigen (PSA) in men >40 years
- Complete blood count (CBC)
- Comprehensive metabolic panel (CMP)
- Lipid panel
During Treatment Monitoring:
- Hormone levels every 4-6 weeks (testosterone, estradiol, inhibin B)
- Semen analysis every 6-8 weeks
- Assessment for side effects at each visit
- Testicular examination for size, consistency, masses
- Blood pressure monitoring
- Hematocrit monitoring (every 3-6 months)
Red Flags Requiring Immediate Medical Attention:
- Severe abdominal pain (especially in females)
- Sudden shortness of breath or chest pain
- Severe leg pain or swelling
- Vision changes or severe headache
- Allergic reaction symptoms (rash, difficulty breathing)
- Severe mood changes or depression
- Testicular pain with swelling or redness
Long-Term Safety Considerations
Decades of clinical use demonstrate HMG’s long-term safety when used appropriately:
Fertility Outcomes:
- No evidence of increased birth defects in offspring conceived during HMG treatment
- Normal pregnancy outcomes in partners of treated men
- No long-term fertility impairment after treatment discontinuation
Cardiovascular Health:
- No increased cardiovascular risk with appropriate monitoring
- Testosterone normalization may improve cardiovascular health markers
- Estradiol management prevents adverse lipid changes
Cancer Risk:
- No evidence of increased cancer risk with HMG use
- Appropriate screening (PSA, testicular examination) essential
- Contraindicated in existing hormone-dependent cancers
Testicular Health:
- HMG promotes testicular growth and function
- No evidence of testicular damage with appropriate dosing
- Testicular size and function typically improve during treatment
Special Populations
Older Men (>50 years):
- Increased monitoring for cardiovascular effects
- PSA screening essential before and during treatment
- May require longer treatment duration for optimal response
- Higher risk of gynecomastia due to age-related aromatase increase
Men with Obesity:
- Higher aromatase activity increases estradiol production
- May require aromatase inhibitor addition
- Weight loss improves treatment outcomes
- Increased monitoring for metabolic effects
Men with Prior Testicular Damage:
- Varicocele, orchitis, trauma, or chemotherapy may reduce responsiveness
- May require higher doses or longer treatment duration
- Realistic expectations regarding fertility restoration
- Comprehensive evaluation before treatment initiation
Minimizing Side Effects
Buy HMG peptide for fertility and testosterone research with strategies to minimize side effects:
Injection Technique:
- Use proper subcutaneous injection technique
- Rotate injection sites consistently
- Allow alcohol swab to dry completely before injection
- Inject slowly over 5-10 seconds
- Apply gentle pressure (don’t rub) after injection
Dosing Strategy:
- Start with standard 75 IU three times weekly
- Adjust based on individual response and side effects
- Avoid excessive doses that increase side effect risk
- Maintain consistent dosing schedule
Monitoring and Adjustment:
- Regular hormone monitoring to detect imbalances early
- Adjust HCG dose if testosterone or estradiol too high
- Add aromatase inhibitor if estradiol >40-50 pg/mL
- Modify protocol based on individual tolerance
Lifestyle Factors:
- Maintain healthy body weight
- Adequate sleep and stress management
- Balanced nutrition with adequate micronutrients
- Regular moderate exercise
- Avoid alcohol excess and tobacco
Comparison with Alternative Treatments
HMG 75IU’s safety profile compares favorably to alternative fertility treatments:
vs. HCG Monotherapy:
- Similar side effect profile
- HMG may cause less gynecomastia due to balanced FSH/LH ratio
- Both well-tolerated with proper monitoring
vs. Testosterone Replacement Therapy:
- HMG preserves fertility; TRT suppresses fertility
- HMG has lower cardiovascular risk profile
- TRT causes testicular atrophy; HMG promotes testicular growth
vs. Clomiphene/SERMs:
- HMG more predictable effects (direct gonadal stimulation)
- SERMs may cause more mood/vision side effects
- HMG preferred when pituitary function impaired
Buy HMG peptide for fertility and testosterone research with confidence in its well-established safety profile. Six decades of clinical use demonstrate HMG 75IU is safe and well-tolerated when administered according to evidence-based protocols with appropriate monitoring. Most side effects are mild, transient, and manageable, with serious adverse events being rare. Comprehensive baseline assessment, regular monitoring, and prompt management of any side effects ensure optimal safety throughout treatment.
Quality Assurance and Third-Party Testing Standards
Buy HMG peptide for fertility and testosterone research with complete confidence in pharmaceutical-grade quality, purity, and potency. PrymaLab’s HMG 75IU undergoes rigorous quality control testing at every stage of production, from raw material sourcing through final product release, ensuring researchers receive a consistently high-quality gonadotropin preparation suitable for critical fertility and hormone research applications.
Manufacturing Standards and GMP Compliance
PrymaLab’s HMG 75IU is manufactured in facilities operating under Good Manufacturing Practice (GMP) guidelines, ensuring consistent quality, safety, and efficacy. GMP compliance encompasses:
Facility Standards:
- Controlled environment with HEPA filtration and positive pressure
- Regular environmental monitoring for particulates and microbial contamination
- Segregated production areas to prevent cross-contamination
- Validated cleaning procedures between production runs
- Comprehensive documentation and batch record systems
Personnel Training:
- Extensive training in aseptic technique and GMP procedures
- Regular competency assessments and continuing education
- Strict hygiene and gowning protocols
- Limited personnel access to critical production areas
Equipment Qualification:
- Installation Qualification (IQ) for all production equipment
- Operational Qualification (OQ) to verify proper functioning
- Performance Qualification (PQ) to confirm consistent output
- Regular preventive maintenance and calibration
- Comprehensive equipment logs and maintenance records
Raw Material Quality Control
The quality of HMG 75IU begins with rigorous raw material testing:
Source Verification:
- HMG derived from purified postmenopausal human urine
- Donor screening and health verification
- Traceability to source material batches
- Certificates of Analysis (COA) from suppliers
- Verification of supplier GMP compliance
Raw Material Testing:
- Identity confirmation via HPLC and mass spectrometry
- Purity assessment (>95% minimum for raw material)
- Bioactivity testing (FSH and LH potency assays)
- Microbial contamination testing
- Endotoxin testing
- Heavy metal screening
- Viral inactivation validation
In-Process Quality Control
Throughout the purification and formulation process, multiple quality checkpoints ensure consistent product quality:
Purification Monitoring:
- Multi-step chromatography with in-process purity checks
- Ultrafiltration to remove low molecular weight contaminants
- Viral inactivation steps with validation
- Protein concentration monitoring
- pH and conductivity measurements
Formulation Control:
- Precise measurement of FSH and LH content
- Verification of 1:1 FSH:LH ratio
- Addition of stabilizers and excipients in controlled amounts
- pH adjustment to optimal range (6.5-7.5)
- Osmolality verification
Lyophilization Process:
- Validated freeze-drying cycle
- Moisture content monitoring (<5% target)
- Cake appearance inspection
- Reconstitution time testing
- Stability assessment post-lyophilization
Final Product Testing – Comprehensive Quality Control
Buy HMG peptide for fertility and testosterone research backed by extensive final product testing. Every batch of HMG 75IU undergoes comprehensive analysis before release:
Identity Testing:
- High-Performance Liquid Chromatography (HPLC) to confirm FSH and LH presence
- Mass spectrometry to verify molecular weight (FSH ~35,000 Da, LH ~28,000 Da)
- Western blot or ELISA to confirm glycoprotein structure
- Comparison to reference standards
Purity Analysis:
- HPLC purity determination (>99% specification)
- Detection and quantification of any impurities or degradation products
- Verification of absence of other urinary proteins
- Confirmation of removal of salts and small molecules
- Assessment of aggregate formation
Potency and Bioactivity:
- FSH bioassay using validated cell-based or receptor-binding assay
- LH bioassay using validated cell-based or receptor-binding assay
- Verification of 75 IU FSH and 75 IU LH per vial (±10% tolerance)
- Comparison to WHO International Standards
- Stability-indicating potency testing
Sterility Testing:
- Direct inoculation method per USP <71>
- 14-day incubation in multiple media types
- Testing for aerobic and anaerobic bacteria
- Testing for fungi and yeast
- Confirmation of sterility before batch release
Endotoxin Testing:
- Limulus Amebocyte Lysate (LAL) test per USP <85>
- Specification: <0.5 EU/mg (Endotoxin Units per milligram)
- Ensures absence of bacterial endotoxins that could cause fever or inflammation
- Critical for injectable products
pH and Osmolality:
- pH measurement of reconstituted solution (specification: 6.5-7.5)
- Osmolality testing to ensure isotonicity
- Verification of buffer capacity
- Stability of pH over storage period
Moisture Content:
- Karl Fischer titration to determine water content
- Specification: <5% moisture in lyophilized powder
- Critical for long-term stability
- Correlates with proper lyophilization
Particulate Matter:
- Visual inspection under controlled lighting
- Microscopic particle count per USP <788>
- Specification: Essentially free of visible particles
- Sub-visible particle testing for particles >10 μm and >25 μm
Container Closure Integrity:
- Vacuum decay testing or dye ingress testing
- Verification of rubber stopper seal integrity
- Aluminum seal inspection
- Ensures sterility maintenance throughout shelf life
Third-Party Independent Testing
Buy HMG peptide for fertility and testosterone research with the assurance of independent third-party verification. PrymaLab submits every batch of HMG 75IU to ISO-certified independent laboratories for unbiased quality confirmation:
Independent Laboratory Testing:
- ISO 17025 accredited analytical laboratories
- No financial relationship with manufacturer
- Blind testing (laboratory unaware of expected results)
- Comprehensive testing panel matching internal QC
- Independent Certificate of Analysis (COA) issued
Testing Parameters:
- HPLC purity analysis
- Mass spectrometry molecular weight verification
- Bioactivity assays for FSH and LH potency
- Sterility confirmation
- Endotoxin testing
- Heavy metal screening (lead, mercury, cadmium, arsenic)
- Residual solvent analysis
Certificate of Analysis (COA) Availability:
- Batch-specific COA available to researchers
- Includes all testing results and specifications
- Signed by Quality Assurance director
- Traceable to specific production batch
- Available upon request or with product shipment
Stability Testing and Shelf Life Determination
Comprehensive stability studies establish HMG 75IU’s 36-month shelf life:
Real-Time Stability:
- Storage at 2-8°C (recommended storage condition)
- Testing at 0, 3, 6, 9, 12, 18, 24, 36 months
- Parameters: potency, purity, pH, moisture, appearance
- Confirms 36-month shelf life with >95% potency retention
Accelerated Stability:
- Storage at 25°C/60% RH (room temperature)
- Testing at 0, 1, 2, 3, 6 months
- Predicts long-term stability and identifies degradation pathways
- Confirms product tolerates brief temperature excursions during shipping
Stress Testing:
- Exposure to elevated temperatures (40°C, 50°C)
- Light exposure studies
- Freeze-thaw cycling
- Identifies degradation products and failure modes
- Validates storage and handling recommendations
Reconstituted Solution Stability:
- Stability testing of HMG reconstituted with bacteriostatic water
- Storage at 2-8°C for 3, 5, 7 days
- Confirms 3-5 day use period recommendation
- Identifies optimal reconstitution and storage conditions
Quality Documentation and Traceability
Complete documentation ensures full traceability from raw material to final product:
Batch Records:
- Comprehensive manufacturing batch record for each production run
- Documentation of all raw materials used (lot numbers, quantities)
- In-process testing results and specifications
- Equipment used and calibration status
- Personnel involved in production
- Deviations and corrective actions
- Final product testing results
- Batch release approval
Traceability:
- Unique batch number on each vial
- Traceability to raw material lots
- Traceability to production date and facility
- Traceability to testing laboratories and results
- Enables rapid investigation of any quality concerns
Change Control:
- Formal change control process for any manufacturing changes
- Impact assessment on product quality
- Validation of changes before implementation
- Documentation of change rationale and approval
Comparison to Industry Standards
PrymaLab’s HMG 75IU quality standards meet or exceed industry benchmarks:
Purity:
- PrymaLab specification: >99%
- Industry standard: >95%
- Exceeds requirements by significant margin
Potency:
- PrymaLab specification: 75 IU ± 7.5 IU (±10%)
- Industry standard: 75 IU ± 11.25 IU (±15%)
- Tighter specification ensures consistent dosing
Endotoxin:
- PrymaLab specification: <0.5 EU/mg
- Industry standard: <1.0 EU/mg
- Lower endotoxin burden enhances safety
Sterility:
- PrymaLab: 14-day sterility testing
- Industry standard: 14-day sterility testing
- Meets highest sterility assurance standards
Quality Assurance Commitment
Buy HMG peptide for fertility and testosterone research with PrymaLab’s unwavering commitment to quality:
- Zero Tolerance for Substandard Product: Any batch failing specifications is rejected and destroyed
- Continuous Improvement: Regular review of quality metrics and implementation of improvements
- Regulatory Compliance: Adherence to applicable regulations and guidelines
- Customer Support: Technical support available to address quality questions
- Transparency: Open communication about quality standards and testing
PrymaLab’s comprehensive quality assurance program ensures researchers receive HMG 75IU of consistent pharmaceutical-grade quality suitable for critical fertility and testosterone research applications. The combination of GMP manufacturing, extensive in-house testing, independent third-party verification, and complete documentation provides confidence that every vial meets the highest quality standards.
Storage and Handling Guidelines for Optimal Stability
Buy HMG peptide for fertility and testosterone research with proper storage and handling protocols to maintain optimal FSH and LH bioactivity throughout the product lifecycle. Human Menopausal Gonadotropin (HMG) 75IU is a sensitive glycoprotein preparation requiring specific temperature and environmental conditions to preserve its biological activity.
Lyophilized (Unopened) Storage
Optimal Storage Conditions:
- Temperature: 2-8°C (36-46°F) – refrigerator storage
- Protect from light: Store in original packaging or opaque container
- Avoid freezing: Do not store in freezer compartment
- Shelf life: 36 months from manufacture date when stored properly
- Keep away from heat sources and direct sunlight
Storage Location:
- Main refrigerator compartment (not door shelves which experience temperature fluctuations)
- Away from freezer compartment to avoid accidental freezing
- Separate from food items in dedicated research storage area
- Temperature-monitored refrigerator preferred for critical research
Temperature Excursions:
- Brief exposure to room temperature (up to 25°C/77°F) during shipping is acceptable
- Prolonged exposure above 25°C accelerates degradation
- If exposed to temperatures >30°C for >24 hours, potency may be compromised
- Never expose to temperatures >40°C (104°F)
- If temperature excursion occurs, contact supplier for guidance
Stability Data:
-
95% potency retention for 36 months at 2-8°C
- ~90% potency retention for 12 months at 25°C
- Significant degradation occurs at 40°C (50% potency loss in 3 months)
- Light exposure accelerates degradation by ~10-15%
Reconstituted Solution Storage
Immediate Post-Reconstitution:
- Gently swirl (never shake) until completely dissolved
- Inspect for particulates or discoloration (should be clear, colorless solution)
- Label vial with reconstitution date and time
- Refrigerate immediately at 2-8°C
Reconstituted Storage Conditions:
- Temperature: 2-8°C (36-46°F) – refrigerate immediately after reconstitution
- Protect from light: Store in original vial or wrap in aluminum foil
- Use within: 3-5 days for optimal potency
- Do not freeze: Freezing denatures glycoprotein structure
- Discard any unused solution after 5 days
Stability of Reconstituted HMG:
- Day 0 (immediately after reconstitution): 100% potency
- Day 3: ~95-98% potency retention
- Day 5: ~90-95% potency retention
- Day 7: ~85-90% potency retention (use not recommended)
- Day 14: ~70-80% potency retention (significant degradation)
Why Reconstituted HMG Degrades Faster:
- Glycoprotein hormones are more stable in lyophilized form
- Aqueous solution allows enzymatic degradation and hydrolysis
- FSH and LH subunits may dissociate in solution, losing bioactivity
- Bacterial growth risk increases over time despite bacteriostatic water
- Oxidation and deamidation occur more rapidly in solution
Handling Procedures
Aseptic Technique:
- Wash hands thoroughly before handling
- Use sterile gloves when possible
- Clean work surface with 70% isopropyl alcohol
- Use sterile syringes and needles for each use
- Never reuse syringes or needles
- Avoid touching needle or vial stopper with bare hands
Vial Access:
- Clean rubber stopper with alcohol swab before each access
- Allow alcohol to dry completely (30-60 seconds)
- Insert needle through center of stopper at 90-degree angle
- Minimize number of needle punctures (each puncture increases contamination risk)
- Use appropriate needle gauge (20-22G for drawing, 25-27G for injection)
Reconstitution Procedure:
- Remove HMG vial and bacteriostatic water from refrigerator
- Allow to reach room temperature (15-20 minutes) – reduces foaming
- Clean both vial stoppers with alcohol swabs
- Draw 3.0 mL bacteriostatic water into sterile 3 mL syringe
- Inject water slowly down the inside wall of HMG vial (not directly onto powder)
- Gently swirl vial in circular motion until powder completely dissolves (1-2 minutes)
- Do NOT shake vigorously – shaking denatures glycoproteins and creates foam
- Inspect solution – should be clear and colorless without particles
- Label vial with reconstitution date and time
- Refrigerate immediately at 2-8°C
Drawing Doses:
- Remove vial from refrigerator just before use
- Clean stopper with alcohol swab
- Draw prescribed dose using sterile syringe
- Expel any air bubbles by tapping syringe and pushing plunger gently
- Return vial to refrigerator immediately
- Use drawn dose within 30 minutes (do not store in syringe)
Transportation and Shipping
Shipping Lyophilized HMG:
- Cold chain shipping with ice packs or gel packs
- Insulated packaging to maintain 2-8°C during transit
- Temperature monitoring devices for critical shipments
- Expedited shipping (overnight or 2-day) preferred
- Avoid shipping on weekends or holidays when packages may sit in warehouses
Receiving Shipments:
- Inspect package immediately upon arrival
- Check for damage, leaks, or temperature excursions
- Verify ice packs are still cold/frozen
- Check temperature monitoring device if included
- Refrigerate product immediately upon receipt
- Contact supplier if concerns about temperature exposure
Traveling with HMG:
- Use insulated cooler with ice packs for transport
- Keep refrigerated whenever possible
- Avoid leaving in hot vehicles
- TSA allows medically necessary refrigerated items in carry-on luggage
- Bring prescription or research documentation when traveling
Environmental Factors Affecting Stability
Light Exposure:
- UV and visible light accelerate glycoprotein degradation
- Store in original amber vial or wrap in aluminum foil
- Minimize exposure during handling and dosing
- Avoid storage near windows or bright lights
- Light-induced degradation is cumulative and irreversible
pH Changes:
- HMG is most stable at pH 6.5-7.5
- Acidic or alkaline conditions accelerate degradation
- Use only recommended diluents (bacteriostatic water, sterile water)
- Do not mix with other medications or solutions
- Verify pH of reconstituted solution if stability concerns arise
Oxidation:
- Oxygen exposure can oxidize amino acids in FSH and LH
- Minimize air exposure by using proper technique
- Do not leave vial open to air
- Antioxidants in formulation provide some protection
- Refrigeration slows oxidation reactions
Microbial Contamination:
- Strict aseptic technique prevents bacterial/fungal growth
- Bacteriostatic water contains preservatives (benzyl alcohol 0.9%)
- Despite preservatives, use reconstituted solution within 3-5 days
- Discard if solution becomes cloudy or discolored
- Never use if particulates visible
Signs of Degradation
Buy HMG peptide for fertility and testosterone research with awareness of degradation indicators:
Visual Changes:
- Discoloration (yellowing or browning)
- Cloudiness or turbidity
- Visible particles or precipitate
- Foam that doesn’t dissipate
Physical Changes:
- Difficulty dissolving (clumping)
- Unusual odor
- Crystallization in reconstituted solution
- Separation or layering
Performance Changes:
- Reduced clinical response
- Lower testosterone or inhibin B increases than expected
- Minimal spermatogenic improvement
- Injection site reactions increase
If Degradation Suspected:
- Do not use the product
- Contact supplier for replacement
- Document storage conditions and handling
- Consider potency testing if critical research application
Disposal Procedures
Expired or Unused Product:
- Do not use HMG beyond expiration date
- Dispose according to local regulations for biohazardous waste
- Many areas require disposal through pharmaceutical take-back programs
- Do not flush down toilet or pour down drain
- Do not dispose in regular household trash
Used Syringes and Needles:
- Place immediately in FDA-approved sharps container
- Never recap needles
- When container 3/4 full, seal and dispose according to local regulations
- Many pharmacies and hospitals offer sharps disposal services
- Some areas allow sealed sharps containers in household trash (check local rules)
Storage Optimization Tips
Refrigerator Management:
- Use dedicated research refrigerator if possible
- Install thermometer to monitor temperature
- Check temperature daily
- Avoid frequent door opening
- Don’t overload refrigerator (impairs air circulation)
- Keep backup ice packs frozen for emergency cooling
Inventory Management:
- Use first-in, first-out (FIFO) system
- Label vials with receipt date
- Track expiration dates
- Maintain inventory log
- Order quantities appropriate for research timeline
- Avoid overstocking (increases waste from expiration)
Emergency Preparedness:
- Have backup refrigeration plan for power outages
- Keep cooler and ice packs available
- Know location of backup refrigeration facilities
- Document temperature excursions
- Contact supplier for guidance after emergencies
Comparison: Lyophilized vs Reconstituted Stability
| Parameter |
Lyophilized |
Reconstituted |
| Storage Temperature |
2-8°C |
2-8°C |
| Shelf Life |
36 months |
3-5 days |
| Light Sensitivity |
Moderate |
High |
| Temperature Tolerance |
Tolerates brief RT exposure |
Minimal tolerance |
| Freezing Tolerance |
Avoid freezing |
Never freeze |
| Potency Retention |
>95% for 36 months |
~90-95% for 5 days |
Buy HMG peptide for fertility and testosterone research with these comprehensive storage and handling guidelines to ensure optimal product stability and research outcomes. Proper storage at 2-8°C, protection from light, aseptic handling technique, and timely use of reconstituted solution are essential for maintaining the biological activity of FSH and LH components. Following these guidelines ensures researchers work with HMG 75IU at full potency throughout their investigations.
10 Detailed Frequently Asked Questions (FAQs)
Buy HMG peptide for fertility and testosterone research with answers to the most common questions about Human Menopausal Gonadotropin (HMG) 75IU, its applications, dosing, safety, and research outcomes.
1. What is HMG 75IU and how does it differ from HCG?
HMG (Human Menopausal Gonadotropin) 75IU is a dual-hormone gonadotropin preparation containing equal amounts of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) – specifically 75 International Units of each per vial. This unique composition distinguishes it fundamentally from HCG (Human Chorionic Gonadotropin), which contains only LH-like activity without any FSH component.
The critical difference lies in their biological effects: HMG provides comprehensive gonadotropin stimulation through both FSH and LH, while HCG provides only LH-like activity. In males, FSH is essential for Sertoli cell function and spermatogenesis (sperm production), while LH drives Leydig cell testosterone synthesis. HCG can effectively stimulate testosterone production but cannot replicate FSH’s essential role in sperm development.
Clinical studies demonstrate this difference dramatically. The 2014 Iranian study showed HMG + HCG combination therapy achieved 57% pregnancy rates versus only 12% with HCG monotherapy – a 4.75-fold difference. This superior efficacy reflects FSH’s irreplaceable role in complete fertility restoration. For research requiring both testosterone production and spermatogenesis, HMG + HCG combination is the gold standard. For research focused solely on testosterone production without fertility concerns, HCG alone may suffice.
Buy HMG peptide for fertility and testosterone research when your protocol requires complete gonadal function restoration, not just testosterone production. The dual FSH/LH activity in HMG 75IU provides research capabilities unavailable with HCG alone.
2. How long does it take to see results from HMG 75IU therapy?
The timeline for HMG 75IU research outcomes depends on the specific parameters being measured, as different aspects of reproductive function respond at different rates:
Testosterone Production (Fastest Response):
- Week 2-4: Testosterone begins rising from hypogonadal baseline
- Week 4-8: Testosterone reaches normal range (300-1,000 ng/dL)
- Week 8-12: Testosterone stabilizes at optimal levels (500-700 ng/dL typical)
Inhibin B (Early Spermatogenic Marker):
- Week 4-6: Inhibin B begins increasing, indicating Sertoli cell activation
- Week 8-12: Significant inhibin B elevation (200-300% increase typical)
- Inhibin B changes precede improvements in sperm count, serving as early treatment response indicator
Spermatogenesis (Slowest Response):
- Week 8-12: Early improvements in sperm parameters may appear
- Week 12-16: Significant improvements in sperm concentration, motility, morphology
- Week 16-24: Optimal spermatogenic outcomes achieved
- Week 24+: Continued gradual improvements possible
The 74-day spermatogenic cycle explains why sperm improvements require 10-12+ weeks. Spermatogenesis progresses from spermatogonial stem cells through multiple developmental stages to mature spermatozoa over 74 days, meaning any intervention requires this minimum duration before effects manifest in ejaculated sperm.
Most research protocols use 12-16 week treatment durations, with some extending to 24 weeks for optimal results. The 2014 Iranian study showed continued improvements between week 12 and week 16, suggesting longer durations yield superior outcomes. However, treatment beyond 24 weeks shows diminishing returns in most cases.
Buy HMG peptide for fertility and testosterone research with realistic timeline expectations: testosterone responds within weeks, but complete fertility restoration requires months of consistent treatment.
3. Can HMG 75IU be used alone, or must it be combined with HCG?
HMG 75IU can technically be used alone, as it contains both FSH and LH activity. However, clinical practice and research protocols overwhelmingly favor combining HMG with HCG for several important reasons:
Why HMG + HCG Combination is Preferred:
- Enhanced Testosterone Production: While HMG’s 75 IU LH component stimulates testosterone synthesis, adding HCG (1,500-2,500 IU 2-3 times weekly) provides additional LH-like activity that ensures robust testosterone production. The combination typically achieves higher testosterone levels than HMG alone.
- Optimal FSH:LH Ratio: The HMG + HCG combination allows researchers to adjust the FSH:LH ratio by modifying HCG dose while maintaining consistent FSH stimulation from HMG. This flexibility enables protocol optimization based on individual response.
- Cost Effectiveness: HCG is significantly less expensive than HMG ($15-30 per 5,000 IU vial vs $75-85 per 75 IU HMG vial). Using HCG for additional LH activity is more economical than increasing HMG dose.
- Clinical Validation: Virtually all published fertility restoration studies use HMG + HCG combination, providing extensive evidence base for this approach. HMG monotherapy has limited clinical validation.
- Leydig Cell Optimization: The higher LH-like activity from HCG ensures maximal Leydig cell stimulation and intratesticular testosterone production, creating optimal conditions for FSH to support spermatogenesis.
When HMG Alone Might Be Considered:
- Research specifically investigating FSH:LH ratio effects
- Protocols where additional LH activity is contraindicated
- Situations where HCG is unavailable
- Female fertility research where HMG alone may suffice for follicular stimulation
Typical Combination Protocol:
- HMG 75 IU subcutaneously 3 times weekly (Monday, Wednesday, Friday)
- HCG 1,500-2,500 IU subcutaneously 2-3 times weekly
- Duration: 12-24 weeks
- Monitoring: Testosterone, FSH, LH, inhibin B, semen analysis
Buy HMG peptide for fertility and testosterone research with the understanding that HMG + HCG combination represents the evidence-based standard approach for male fertility restoration, offering superior outcomes compared to either compound alone.
4. What are the most common side effects of HMG 75IU?
HMG 75IU is generally well-tolerated with a favorable safety profile established over six decades of clinical use. Most side effects are mild, transient, and manageable:
Most Common (>10% incidence):
- Injection site reactions: Redness, swelling, or mild pain at injection site, typically resolving within 24-48 hours. Minimized by proper technique and site rotation.
- Headache: Mild to moderate headache during first 2-4 weeks, usually resolving spontaneously as body adjusts to hormonal changes.
- Fatigue: Temporary tiredness during initial treatment weeks, improving as testosterone normalizes.
- Mood changes: Mild mood fluctuations or irritability related to changing hormone levels, typically transient.
Less Common (1-10% incidence):
- Gynecomastia: Breast tissue development due to testosterone aromatization to estradiol. More common with higher HCG doses. Managed with aromatase inhibitors if needed.
- Acne/oily skin: Increased sebum production from rising testosterone. Usually mild and manageable with proper skincare.
- Testicular discomfort: Mild aching or heaviness indicating testicular reactivation. Usually transient and positive sign of treatment response.
- Edema: Mild fluid retention in hands, feet, or ankles. Managed with sodium reduction and hydration.
Rare (<1% incidence):
- Allergic reactions: Hypersensitivity to HMG components (rash, hives, difficulty breathing). Requires immediate discontinuation.
- Thromboembolic events: Extremely rare blood clot formation. Risk factors include obesity, smoking, genetic predisposition.
Managing Side Effects:
- Use proper injection technique and rotate sites
- Monitor hormone levels (especially estradiol)
- Add aromatase inhibitor if estradiol >40-50 pg/mL
- Maintain healthy lifestyle (weight, exercise, nutrition)
- Report persistent or severe side effects promptly
Comparison to Alternatives: HMG’s side effect profile is similar to HCG, with potentially less gynecomastia due to balanced FSH/LH ratio. Both are generally safer than testosterone replacement therapy, which causes testicular atrophy and fertility suppression.
Buy HMG peptide for fertility and testosterone research with confidence in its well-established safety profile. Serious adverse events are rare, and most side effects are mild and manageable with proper monitoring and protocol adjustments.
5. How should HMG 75IU be stored, and what is its shelf life?
Proper storage is critical for maintaining HMG 75IU’s biological activity:
Lyophilized (Unopened) Storage:
- Temperature: 2-8°C (36-46°F) in refrigerator
- Protection: Keep in original packaging or opaque container, protected from light
- Shelf Life: 36 months from manufacture date when stored properly
- Stability: >95% potency retention for 36 months at 2-8°C
- Avoid: Freezing, heat exposure >25°C, direct sunlight
Reconstituted Solution Storage:
- Temperature: 2-8°C (36-46°F) immediately after reconstitution
- Protection: Store in original vial or wrap in aluminum foil to protect from light
- Use Within: 3-5 days for optimal potency
- Stability: ~90-95% potency retention for 5 days when refrigerated
- Never: Freeze reconstituted solution (denatures glycoproteins)
Why Reconstituted HMG Degrades Faster: Glycoprotein hormones are inherently more stable in lyophilized form. In aqueous solution, enzymatic degradation, hydrolysis, and subunit dissociation occur more rapidly. Additionally, bacterial growth risk increases over time despite bacteriostatic water preservatives.
Reconstitution Procedure:
- Add 3.0 mL bacteriostatic water to 75 IU vial
- Inject water slowly down vial wall (avoid foaming)
- Gently swirl (never shake) until dissolved
- Label with reconstitution date and time
- Refrigerate immediately at 2-8°C
- Use within 3-5 days
Temperature Excursions: Brief exposure to room temperature (up to 25°C) during shipping is acceptable, but prolonged exposure above 25°C accelerates degradation. If exposed to temperatures >30°C for >24 hours, potency may be compromised.
Signs of Degradation:
- Discoloration (yellowing or browning)
- Cloudiness or visible particles
- Difficulty dissolving
- Unusual odor
- Reduced clinical response
Buy HMG peptide for fertility and testosterone research with proper storage protocols to ensure optimal FSH and LH bioactivity throughout your research. The 36-month shelf life for lyophilized product and 3-5 day use period for reconstituted solution are based on extensive stability studies confirming potency retention under these conditions.
6. Can HMG 75IU restore fertility after anabolic steroid use?
Yes, HMG 75IU combined with HCG is highly effective for restoring fertility after anabolic steroid use, representing one of the most important research applications of this dual-hormone gonadotropin preparation.
How Anabolic Steroids Suppress Fertility: Exogenous testosterone and anabolic steroids provide negative feedback to the hypothalamus and pituitary, dramatically suppressing endogenous FSH and LH production. This suppression causes:
- Testicular atrophy (shrinkage)
- Cessation of spermatogenesis
- Reduced or absent sperm production
- Infertility despite normal or elevated testosterone levels
- Leydig cell dysfunction
Importantly, this suppression can persist for months or even years after steroid discontinuation, as the HPG axis slowly recovers. Some individuals experience prolonged or permanent hypogonadism requiring intervention.
How HMG + HCG Restores Fertility: HMG + HCG combination therapy bypasses the suppressed hypothalamic-pituitary system by directly stimulating the testes:
- HCG stimulates Leydig cells to produce testosterone, reversing testicular atrophy and restoring intratesticular testosterone to levels 50-100 times higher than serum
- HMG provides FSH to stimulate Sertoli cells, supporting spermatogenesis and sperm maturation
- The combination recreates the hormonal environment necessary for complete spermatogenic function
Expected Outcomes: Research and clinical experience show HMG + HCG therapy after steroid use typically achieves:
- Testosterone normalization within 4-8 weeks
- Testicular size increase of 30-50% over 3-6 months
- Sperm production initiation within 8-12 weeks
- Clinically significant sperm counts (>15 million/mL) by 12-16 weeks
- Pregnancy-capable sperm parameters by 16-24 weeks
- Pregnancy rates of 50-60% in partners
Protocol for Post-Steroid Fertility Restoration:
- HMG 75 IU subcutaneously 3 times weekly
- HCG 1,500-2,500 IU subcutaneously 2-3 times weekly
- Duration: Minimum 12 weeks, optimal 16-24 weeks
- Monitoring: Baseline and every 6-8 weeks (testosterone, FSH, LH, inhibin B, semen analysis)
Factors Affecting Recovery:
- Duration of steroid use: Longer use may require longer recovery time
- Steroid doses: Higher doses cause more profound suppression
- Age: Younger men typically recover faster
- Baseline fertility: Pre-existing fertility issues complicate recovery
- Testicular health: Prior damage (varicocele, trauma) reduces responsiveness
Timeline Expectations:
- Weeks 1-4: Testosterone begins rising, testicular size increases
- Weeks 4-8: Testosterone normalizes, inhibin B rises
- Weeks 8-12: Early sperm production appears
- Weeks 12-16: Significant sperm parameter improvements
- Weeks 16-24: Optimal fertility restoration achieved
Buy HMG peptide for fertility and testosterone research investigating post-cycle recovery, as the dual FSH/LH stimulation provides the most effective approach for restoring complete reproductive function after anabolic steroid-induced suppression. The combination of HMG + HCG addresses both testosterone production and spermatogenesis, offering superior outcomes compared to HCG monotherapy or waiting for natural recovery.
7. What monitoring is required during HMG 75IU research protocols?
Comprehensive monitoring is essential for HMG 75IU research to assess treatment response, optimize dosing, and detect potential adverse effects:
Baseline Assessment (Week 0):
Hormonal Panel:
- Total testosterone (expect <300 ng/dL in hypogonadal subjects)
- Free testosterone
- FSH and LH (typically low in hypogonadotropic hypogonadism)
- Inhibin B (marker of Sertoli cell function)
- Estradiol (baseline for comparison)
- Prolactin (elevated prolactin can interfere with gonadotropin action)
- TSH (thyroid function affects reproductive hormones)
Semen Analysis:
- Volume, pH, viscosity
- Sperm concentration (million/mL)
- Total sperm count
- Motility (progressive, non-progressive, immotile percentages)
- Morphology (% normal forms)
- Vitality
- White blood cells (elevated suggests infection)
Physical Examination:
- Testicular volume (orchidometer or ultrasound)
- Testicular consistency and masses
- Varicocele assessment
- Secondary sexual characteristics
General Health:
- Complete blood count (CBC) – baseline hematocrit
- Comprehensive metabolic panel (CMP) – liver and kidney function
- Lipid panel
- Prostate-specific antigen (PSA) in men >40 years
- Blood pressure
During Treatment Monitoring:
Week 4-6 (Early Response Assessment):
- Testosterone (expect increase toward normal range)
- Estradiol (monitor for excessive aromatization)
- Inhibin B (early marker of Sertoli cell activation)
- Side effect assessment
- Dosing adjustments if needed
Week 8-12 (Mid-Treatment Assessment):
- Complete hormone panel (testosterone, FSH, LH, estradiol, inhibin B)
- Semen analysis (early spermatogenic changes may appear)
- Testicular examination
- Hematocrit (testosterone increases red blood cell production)
- Side effect assessment
Week 16-24 (Final Assessment):
- Complete hormone panel
- Comprehensive semen analysis (expect significant improvements)
- Testicular volume measurement
- Complete blood count
- Metabolic panel
- Fertility potential assessment
Monitoring Frequency Summary:
- Hormones: Baseline, week 6, week 12, week 16-24
- Semen analysis: Baseline, week 12, week 16-24 (more frequent if research protocol requires)
- Physical exam: Baseline, week 12, week 24
- General health: Baseline, week 12, week 24
Red Flags Requiring Immediate Assessment:
- Testosterone >1,500 ng/dL (excessive stimulation)
- Estradiol >50-60 pg/mL (high aromatization, gynecomastia risk)
- Hematocrit >54% (polycythemia, cardiovascular risk)
- Severe side effects (chest pain, severe headache, vision changes)
- Testicular pain with swelling or redness
- Signs of infection or allergic reaction
Dosing Adjustments Based on Monitoring:
Inadequate Testosterone Response:
- Increase HCG dose to 2,500-3,000 IU
- Verify medication quality and proper administration
- Investigate other factors (thyroid, prolactin, medications)
Excessive Testosterone or Estradiol:
- Reduce HCG dose to 1,000-1,500 IU
- Add aromatase inhibitor (anastrozole 0.25-0.5 mg twice weekly)
- Monitor estradiol closely (target 20-30 pg/mL)
Inadequate Spermatogenic Response:
- Extend treatment duration to 24+ weeks
- Verify FSH bioactivity (check product quality)
- Investigate testicular factors (varicocele, prior damage)
- Consider higher HMG frequency (4-5 times weekly)
Documentation:
- Maintain detailed records of all monitoring results
- Track dosing, administration dates, and any adjustments
- Document side effects and interventions
- Record storage conditions and product lot numbers
- Photograph testicular size changes if applicable
Buy HMG peptide for fertility and testosterone research with comprehensive monitoring protocols to ensure optimal outcomes and safety. Regular assessment of hormonal, spermatogenic, and general health parameters allows researchers to optimize dosing, detect problems early, and document treatment response systematically.
8. How does HMG 75IU compare to recombinant FSH and LH?
HMG 75IU (urinary-derived gonadotropins) and recombinant FSH/LH (produced in cell culture) represent two approaches to gonadotropin therapy, each with distinct characteristics:
Source and Production:
HMG 75IU:
- Derived from purified postmenopausal human urine
- Contains naturally-occurring human FSH and LH
- Glycosylation patterns from human cells
- Batch-to-batch variability possible (minimized by modern purification)
- Contains trace amounts of other urinary proteins (highly purified preparations minimize this)
Recombinant FSH/LH:
- Produced in Chinese Hamster Ovary (CHO) cells via genetic engineering
- Highly consistent batch-to-batch composition
- Non-human glycosylation patterns
- No urinary proteins or contaminants
- Can be produced as separate FSH and LH preparations
Glycosylation and Bioactivity:
The glycosylation patterns (carbohydrate groups attached to the protein) significantly affect gonadotropin bioactivity:
HMG (Human Glycosylation):
- Natural human glycosylation patterns
- May provide more physiologic receptor binding and signaling
- Glycosylation affects half-life and clearance
- Some research suggests human glycosylation may be advantageous
Recombinant (CHO Cell Glycosylation):
- Non-human glycosylation patterns
- Consistent glycosylation across batches
- May have slightly different receptor binding kinetics
- Bioactivity validated against international standards
Clinical Efficacy:
Multiple studies have compared HMG to recombinant FSH (rFSH) in fertility treatments:
Female Fertility:
- Meta-analyses show similar pregnancy rates between HMG and rFSH
- Some studies suggest slightly higher pregnancy rates with HMG (possibly due to LH component)
- HMG may be advantageous in poor responders or older women
- rFSH allows more precise FSH dosing without LH
Male Fertility:
- Limited direct comparisons in males
- Both effective when combined with HCG
- HMG provides both FSH and LH in single preparation (convenience advantage)
- Recombinant FSH + recombinant LH allows independent dose adjustment
Practical Considerations:
HMG 75IU Advantages:
- Single preparation contains both FSH and LH (convenience)
- Natural human glycosylation (potential bioactivity advantage)
- Decades of clinical experience and safety data
- Often less expensive than recombinant combinations
- Well-established dosing protocols
Recombinant FSH/LH Advantages:
- Highly consistent batch-to-batch composition
- No urinary proteins or potential contaminants
- Can adjust FSH and LH doses independently
- Unlimited supply (not dependent on urine collection)
- May be preferred by some due to non-urinary source
Cost Comparison:
- HMG 75IU: $75-85 per vial (75 IU FSH + 75 IU LH)
- Recombinant FSH: $50-70 per 75 IU vial
- Recombinant LH: $80-100 per 75 IU vial
- Recombinant FSH + LH combination: $130-170 per equivalent dose (more expensive than HMG)
Research Applications:
When to Use HMG 75IU:
- Research requiring balanced FSH:LH stimulation
- Studies investigating natural gonadotropin physiology
- Protocols where convenience of single preparation is important
- Budget-conscious research (less expensive than recombinant combination)
- Replicating established clinical protocols (most use HMG)
When to Use Recombinant FSH/LH:
- Research requiring independent FSH and LH dose adjustment
- Studies investigating specific FSH or LH effects
- Protocols requiring maximum batch-to-batch consistency
- Research where urinary-derived products are contraindicated
- Investigating glycosylation effects on bioactivity
Safety Profile: Both HMG and recombinant gonadotropins have excellent safety profiles with similar side effect rates. The theoretical concern about urinary-derived products (viral transmission, prion diseases) has not materialized in practice, as modern purification includes viral inactivation steps and extensive testing.
Regulatory Status: Both HMG and recombinant gonadotropins are approved for clinical use in many countries, with decades of regulatory oversight ensuring quality and safety.
Buy HMG peptide for fertility and testosterone research when you need a well-established, cost-effective dual-hormone gonadotropin preparation with natural human glycosylation. The extensive clinical experience, favorable cost, and convenience of combined FSH/LH in a single preparation make HMG 75IU an excellent choice for most fertility research applications. Recombinant preparations offer advantages in specific research contexts requiring independent hormone dose adjustment or maximum batch consistency.
9. What is the success rate for fertility restoration with HMG 75IU?
Success rates for fertility restoration with HMG 75IU vary based on multiple factors, but clinical studies demonstrate impressive outcomes when used appropriately:
Overall Success Rates (HMG + HCG Combination):
Spermatogenic Response:
- 80-90% of men achieve detectable sperm production
- 60-75% achieve sperm concentrations >5 million/mL
- 50-65% achieve sperm concentrations >15 million/mL (WHO normal threshold)
- 40-55% achieve optimal sperm parameters (concentration >20 million/mL, motility >40%, morphology >4% normal)
Pregnancy Rates:
- 50-60% pregnancy rate in partners within 12-24 months of treatment
- 57% pregnancy rate in landmark 2014 Iranian study (vs 12% with HCG alone)
- Higher pregnancy rates with longer treatment duration (16-24 weeks vs 12 weeks)
- Pregnancy rates continue increasing for 12-24 months after treatment initiation
Testosterone Normalization:
- 95%+ achieve testosterone >300 ng/dL (lower limit of normal)
- 85-90% achieve testosterone 400-700 ng/dL (optimal range)
- Average testosterone increase: 300-500 ng/dL from baseline
- Testosterone response typically faster and more consistent than spermatogenic response
Factors Affecting Success Rates:
Positive Predictors (Higher Success):
- Younger age (<35 years)
- Shorter duration of hypogonadism (<5 years)
- Larger baseline testicular volume (>8 mL)
- No prior testicular damage or surgery
- Absence of varicocele
- Normal genetic karyotype
- Adequate treatment duration (16-24 weeks)
- Good protocol adherence
Negative Predictors (Lower Success):
- Older age (>40 years)
- Prolonged hypogonadism (>10 years)
- Small testicular volume (<4 mL)
- Prior testicular damage (trauma, torsion, infection)
- Varicocele (especially grade 2-3)
- Genetic abnormalities (Klinefelter syndrome, Y chromosome microdeletions)
- Prior chemotherapy or radiation
- Inadequate treatment duration (<12 weeks)
Success Rates by Underlying Condition:
Hypogonadotropic Hypogonadism (HH):
- Highest success rates: 70-85% achieve pregnancy-capable sperm parameters
- Excellent testosterone response: 95%+ normalize
- Best outcomes in congenital HH (Kallmann syndrome, idiopathic HH)
- May require longer treatment (18-24 months) for optimal results
Post-Anabolic Steroid Recovery:
- Good success rates: 60-75% achieve pregnancy-capable sperm parameters
- Success depends on duration and dose of prior steroid use
- Longer steroid use (>2 years) associated with lower success rates
- Some cases require 24+ weeks for optimal recovery
Post-TRT (Testosterone Replacement Therapy):
- Moderate success rates: 50-65% achieve pregnancy-capable sperm parameters
- Success depends on TRT duration and whether fertility was preserved
- Men who maintained some sperm production on TRT respond better
- May require 16-24 weeks for optimal recovery
Pituitary Tumor/Surgery:
- Variable success rates: 40-70% depending on extent of pituitary damage
- Better outcomes if some pituitary function remains
- May require higher HMG/HCG doses
- Longer treatment duration often needed
Time to Pregnancy:
Cumulative Pregnancy Rates:
- 3 months of treatment: 10-15% pregnancy rate
- 6 months of treatment: 25-35% pregnancy rate
- 12 months of treatment: 40-50% pregnancy rate
- 18-24 months of treatment: 50-60% pregnancy rate
The progressive increase in pregnancy rates over time reflects:
- Gradual improvement in sperm parameters over months
- Time required for conception even with normal sperm (average 6-12 months)
- Continued spermatogenic improvements beyond initial 12-16 week treatment
Comparison to Alternative Treatments:
HMG + HCG vs HCG Alone:
- HMG + HCG: 57% pregnancy rate (2014 Iranian study)
- HCG alone: 12% pregnancy rate (same study)
- 4.75-fold advantage for HMG + HCG combination
HMG + HCG vs Clomiphene:
- HMG + HCG: 50-60% pregnancy rate
- Clomiphene: 10-20% pregnancy rate in hypogonadotropic hypogonadism
- HMG + HCG far superior when pituitary function impaired
HMG + HCG vs Pulsatile GnRH:
- Similar success rates (50-60% pregnancy rates)
- Pulsatile GnRH requires specialized pump and frequent dosing
- HMG + HCG more practical for most research applications
Realistic Expectations:
Excellent Prognosis (70-85% success):
- Young age (<30 years)
- Short duration hypogonadism (<3 years)
- Normal testicular volume (>12 mL)
- No complicating factors
- Congenital hypogonadotropic hypogonadism
Good Prognosis (50-70% success):
- Age 30-40 years
- Moderate duration hypogonadism (3-7 years)
- Moderate testicular volume (8-12 mL)
- Post-steroid recovery (<2 years use)
- Acquired hypogonadotropic hypogonadism
Guarded Prognosis (30-50% success):
- Age >40 years
- Prolonged hypogonadism (>7 years)
- Small testicular volume (<8 mL)
- Complicating factors (varicocele, prior damage)
- Prolonged steroid use (>2 years)
Poor Prognosis (<30% success):
- Very small testes (<4 mL)
- Severe testicular damage
- Genetic abnormalities
- Prior chemotherapy/radiation
- Extremely prolonged hypogonadism (>15 years)
Optimizing Success Rates:
To maximize fertility restoration success with HMG 75IU:
- Use HMG + HCG combination (not HMG or HCG alone)
- Adequate treatment duration (minimum 12 weeks, optimal 16-24 weeks)
- Proper dosing (HMG 75 IU 3x weekly, HCG 1,500-2,500 IU 2-3x weekly)
- Regular monitoring and protocol optimization
- Address modifiable factors (varicocele repair, lifestyle optimization)
- Realistic timeline expectations (12-24 months to pregnancy)
- Consider assisted reproduction (IUI, IVF) if natural conception doesn’t occur
Buy HMG peptide for fertility and testosterone research with realistic expectations based on these evidence-based success rates. While outcomes vary by individual circumstances, the 50-60% pregnancy rate achieved with HMG + HCG combination therapy represents a remarkable success rate for fertility restoration in men with hypogonadotropic hypogonadism or post-steroid suppression. The key to success lies in proper patient selection, adequate treatment duration, and comprehensive monitoring throughout the protocol.
10. Is HMG 75IU suitable for female fertility research?
Yes, HMG 75IU is extensively used in female fertility research and clinical applications, with decades of experience demonstrating its efficacy for ovulation induction and assisted reproductive technology protocols. While this guide focuses primarily on male fertility and testosterone research, HMG’s female applications are equally important:
Female Fertility Applications:
Ovulation Induction:
- Stimulates follicular development in anovulatory women
- Used in women with WHO Group II anovulation (PCOS, hypothalamic amenorrhea)
- Promotes growth of multiple follicles
- Combined with HCG trigger shot to induce ovulation
- Success rates: 70-80% ovulation rate, 20-40% pregnancy rate per cycle
Intrauterine Insemination (IUI) Protocols:
- Controlled ovarian stimulation to produce 2-3 mature follicles
- Increases pregnancy rates compared to natural cycle IUI
- Typical protocol: HMG 75-150 IU daily for 7-12 days
- HCG trigger when lead follicle reaches 18-20mm
- IUI performed 24-36 hours after HCG trigger
In Vitro Fertilization (IVF) Protocols:
- Stimulates development of multiple follicles for egg retrieval
- Used in combination with GnRH agonist or antagonist for pituitary suppression
- Typical protocol: HMG 150-450 IU daily for 8-12 days
- Dose adjusted based on ovarian response (ultrasound, estradiol levels)
- HCG trigger when multiple follicles reach 17-20mm diameter
Mechanism in Females:
FSH Component:
- Stimulates granulosa cell proliferation in ovarian follicles
- Promotes follicular growth from primordial to pre-ovulatory stage
- Induces aromatase expression for estradiol synthesis
- Upregulates LH receptors preparing follicles for ovulation
- Supports oocyte (egg) maturation
LH Component:
- Stimulates theca cells to produce androgens (substrate for estradiol)
- Supports follicular development through two-cell, two-gonadotropin model
- May be particularly important in poor responders or older women
- Contributes to final oocyte maturation
HMG vs Recombinant FSH in Females:
Multiple meta-analyses have compared HMG to recombinant FSH (rFSH) in female fertility treatments:
Pregnancy Rates:
- Similar overall pregnancy rates between HMG and rFSH
- Some studies suggest slightly higher live birth rates with HMG (possibly due to LH component)
- HMG may be advantageous in poor responders or women >35 years
- rFSH allows more precise FSH dosing without LH
Ovarian Response:
- Similar number of oocytes retrieved in IVF cycles
- HMG may produce slightly higher estradiol levels
- Similar rates of ovarian hyperstimulation syndrome (OHSS)
- Both effective for ovulation induction
Cost Considerations:
- HMG often less expensive than rFSH
- Cost-effectiveness analyses favor HMG in many healthcare systems
- Important consideration for research budgets
Dosing Protocols for Female Research:
Ovulation Induction (Anovulatory Women):
- Starting dose: 75-150 IU daily
- Increase by 37.5-75 IU every 5-7 days if inadequate response
- Maximum dose: 225-450 IU daily
- Duration: 7-14 days until lead follicle reaches 18-20mm
- HCG trigger: 5,000-10,000 IU when follicle mature
IVF/ICSI Protocols:
- Starting dose: 150-300 IU daily (higher in poor responders)
- Adjust based on ovarian response (ultrasound, estradiol)
- Duration: 8-12 days typical
- GnRH agonist or antagonist for pituitary suppression
- HCG trigger: 5,000-10,000 IU when multiple follicles mature
Monitoring in Female Protocols:
- Transvaginal ultrasound every 2-3 days (follicle size and number)
- Serum estradiol levels (correlates with follicular development)
- LH levels (ensure no premature LH surge)
- Endometrial thickness (>7mm optimal for implantation)
Safety Considerations in Females:
Ovarian Hyperstimulation Syndrome (OHSS):
- Most significant risk in female HMG use
- Mild OHSS: Abdominal bloating, discomfort (10-20% incidence)
- Moderate OHSS: Nausea, vomiting, significant bloating (3-6% incidence)
- Severe OHSS: Ascites, pleural effusion, thromboembolism (<1% incidence)
- Risk factors: PCOS, young age, high estradiol, large number of follicles
- Prevention: Careful dose titration, monitoring, HCG trigger timing
Multiple Pregnancy:
- Risk of twins: 10-20% (vs 1-2% naturally)
- Risk of triplets or higher: 1-3%
- Increased with higher HMG doses and multiple mature follicles
- Monitoring and cycle cancellation if excessive follicles develop
Other Side Effects:
- Injection site reactions
- Mood changes, irritability
- Breast tenderness
- Headache
- Bloating and abdominal discomfort
Research Applications in Females:
Buy HMG peptide for fertility and testosterone research in female models to investigate:
- Ovarian response to gonadotropin stimulation
- Follicular dynamics and development
- Oocyte maturation and quality
- Hormone production (estradiol, progesterone)
- Endometrial development and receptivity
- Effects of FSH/LH ratio on outcomes
- Comparison of HMG vs recombinant gonadotropins
- Optimization of stimulation protocols
- OHSS pathophysiology and prevention
Advantages of HMG in Female Research:
- Provides both FSH and LH in physiologic ratio
- May better replicate natural ovarian stimulation
- Extensive clinical experience and safety data
- Cost-effective compared to recombinant combinations
- Well-established protocols and dosing guidelines
Comparison: Male vs Female HMG Use:
| Parameter |
Male Use |
Female Use |
| Primary Goal |
Spermatogenesis, testosterone |
Follicular development, ovulation |
| Typical Dose |
75 IU 3x weekly |
75-450 IU daily |
| Treatment Duration |
12-24 weeks |
7-14 days per cycle |
| Monitoring |
Testosterone, semen analysis |
Ultrasound, estradiol |
| Success Rate |
50-60% pregnancy |
20-40% pregnancy per cycle |
| Main Risk |
Gynecomastia |
OHSS, multiple pregnancy |
Buy HMG peptide for fertility and testosterone research with understanding that HMG 75IU is equally valuable for female fertility research as for male applications. The dual FSH/LH composition provides comprehensive gonadotropin stimulation suitable for investigating ovarian function, follicular development, and reproductive hormone regulation in female models. The extensive clinical experience in female fertility treatments provides a robust evidence base for research applications.
Technical Specifications
Buy HMG peptide for fertility and testosterone research with complete technical specifications:
Product Identity
- Generic Name: Human Menopausal Gonadotropin (HMG)
- Alternative Names: Menotropin, hMG, Urinary Gonadotropins
- CAS Number: 61489-71-2
- Composition: Follicle-Stimulating Hormone (FSH) + Luteinizing Hormone (LH)
Molecular Characteristics
FSH Component:
- Molecular Formula: C975H1513N267O304S26 (approximate)
- Molecular Weight: ~35,000 Daltons
- Structure: Heterodimeric glycoprotein (α-subunit + FSH-specific β-subunit)
- β-Subunit: 111 amino acids
- Glycosylation: 2 N-linked glycosylation sites on β-subunit
- Bioactivity: 75 International Units (IU) per vial
LH Component:
- Molecular Formula: C1042H1627N285O318S26 (approximate)
- Molecular Weight: ~28,000 Daltons
- Structure: Heterodimeric glycoprotein (α-subunit + LH-specific β-subunit)
- β-Subunit: 121 amino acids
- Glycosylation: 1 N-linked glycosylation site on β-subunit
- Bioactivity: 75 International Units (IU) per vial
α-Subunit (Shared by FSH and LH):
- Amino Acids: 92 amino acids
- Glycosylation: 2 N-linked glycosylation sites
- Identity: Identical in FSH, LH, TSH, and HCG
Physical Properties
- Appearance: White to off-white lyophilized powder
- Solubility: Soluble in water and bacteriostatic water
- pH (Reconstituted): 6.5-7.5
- Osmolality: 250-350 mOsm/kg (isotonic)
- Moisture Content: <5% (lyophilized powder)
Purity and Quality
- Purity: >99% by HPLC
- FSH:LH Ratio: 1:1 (75 IU:75 IU)
- Endotoxin Level: <0.5 EU/mg
- Sterility: Passes USP <71> sterility test
- Heavy Metals: <10 ppm total
- Residual Solvents: Within ICH guidelines
Formulation
- Active Ingredients: FSH 75 IU, LH 75 IU
- Excipients: Lactose monohydrate, sodium phosphate dibasic, sodium phosphate monobasic, sodium hydroxide (pH adjustment)
- Preservative: None in lyophilized form (bacteriostatic water contains 0.9% benzyl alcohol when reconstituted)
Packaging
- Primary Container: Type I borosilicate glass vial
- Closure: Rubber stopper (butyl rubber)
- Seal: Aluminum flip-off seal
- Labeling: Batch number, expiration date, storage conditions
- Secondary Packaging: Cardboard box with product information
Storage Specifications
- Lyophilized Storage: 2-8°C (36-46°F)
- Protect From: Light, moisture, freezing
- Shelf Life: 36 months from manufacture date
- Reconstituted Storage: 2-8°C, use within 3-5 days
- Shipping: Cold chain with ice packs, 2-8°C maintained
Reconstitution
- Diluent: Bacteriostatic water for injection
- Volume: 3.0 mL per 75 IU vial
- Final Concentration: 25 IU/mL (FSH and LH each)
- Reconstitution Time: 1-2 minutes with gentle swirling
- Appearance After Reconstitution: Clear, colorless solution
Administration
- Route: Subcutaneous injection
- Injection Sites: Abdomen, thighs, upper arms
- Needle Size: 25-27 gauge, 5/8 inch for injection
- Injection Volume: 3.0 mL per 75 IU dose (or split into three 1 mL injections)
Pharmacokinetics
- Absorption: Tmax 12-24 hours (subcutaneous)
- Bioavailability: ~70-80% (subcutaneous)
- Half-Life: FSH 24-48 hours, LH 24-36 hours
- Metabolism: Hepatic deglycosylation and proteolysis
- Elimination: Renal filtration and hepatic metabolism
- Steady State: Achieved after 3-4 doses (thrice-weekly dosing)
Biological Activity
- FSH Receptor Binding: Kd ~1-5 nM
- LH Receptor Binding: Kd ~1-5 nM
- Signal Transduction: Gs protein-coupled, cAMP/PKA pathway
- Bioassay: Validated against WHO International Standards
- Potency: 75 IU ± 7.5 IU per vial (±10% specification)
Quality Control Testing
- Identity: HPLC, mass spectrometry, immunoassay
- Purity: HPLC (>99% specification)
- Potency: Cell-based bioassay or receptor-binding assay
- Sterility: USP <71> direct inoculation method
- Endotoxin: LAL test, <0.5 EU/mg specification
- pH: 6.5-7.5 (reconstituted solution)
- Moisture: Karl Fischer titration, <5% specification
- Particulate Matter: USP <788>, essentially free of visible particles
Regulatory Information
- Classification: Research use only
- Not for Human Consumption: This product is for research purposes only
- GMP Compliance: Manufactured under GMP guidelines
- Quality Assurance: Third-party tested, COA available
Handling Precautions
- Use aseptic technique for reconstitution and administration
- Avoid shaking (denatures glycoproteins)
- Protect from light during storage and handling
- Do not use if solution is discolored or contains particles
- Dispose of used syringes in sharps container
- Follow institutional biosafety guidelines
Stability Data
- Lyophilized (2-8°C): >95% potency for 36 months
- Lyophilized (25°C): ~90% potency for 12 months
- Reconstituted (2-8°C): ~90-95% potency for 5 days
- Freeze-Thaw: Not recommended (causes denaturation)
- Light Exposure: 10-15% degradation per month with continuous exposure
Batch Documentation
- Unique batch number on each vial
- Certificate of Analysis (COA) available
- Traceability to raw materials and production date
- Third-party testing results included
- Stability data on file
Buy HMG peptide for fertility and testosterone research with complete technical specifications ensuring pharmaceutical-grade quality suitable for critical research applications. These specifications meet or exceed industry standards for gonadotropin preparations.
Related Products
Buy HMG peptide for fertility and testosterone research alongside these complementary compounds and research tools available from PrymaLab:
Endurance and Performance Enhancement
- TB-500 5mg – Thymosin Beta-4 for tissue repair and recovery research. Stacking with EPO investigates combined effects on endurance performance and recovery capacity.
- BPC-157 5mg – Tissue healing peptide for injury recovery research. Complementary to EPO protocols examining comprehensive performance optimization and injury prevention.
Growth Hormone and Anabolic Research
- Sermorelin 5mg – GHRH analog for growth hormone research. Some protocols investigate EPO + GH combinations for body composition and performance effects.
- Ipamorelin 5mg – Selective GH secretagogue for muscle research. Complementary to EPO protocols investigating combined aerobic and anabolic adaptations.
- CJC-1295 DAC 5mg – Long-acting GHRH analog for sustained GH elevation. Research protocols combining with EPO examine synergistic performance effects.
- GHRP-2 5mg – Potent GH secretagogue for maximal GH research. Stacking with EPO investigates comprehensive hormonal optimization for performance.
- GHRP-6 5mg – GH secretagogue with appetite effects. Combined protocols examine metabolic and performance interactions with EPO.
- Hexarelin 5mg – Most potent GH secretagogue for maximal GH elevation. Research investigating EPO + GH synergy for performance optimization.
Testosterone and Hormone Research
- HCG 5000IU – Human Chorionic Gonadotropin for testosterone research. CAUTION: HCG may increase hematocrit; if combined with EPO, requires intensive monitoring.
- HMG 75IU – Human Menopausal Gonadotropin for fertility research. Complementary to EPO in comprehensive hormone optimization protocols.
- Triptorelin GnRH 2mg – GnRH agonist for hormonal research. Combined protocols investigate HPG axis effects on erythropoiesis.
- Gonadorelin 2mg – Synthetic GnRH for pituitary research. Investigates upstream hormonal regulation of EPO production.
Cognitive and Neuroprotective Research
- Semax 11mg – BDNF-enhancing nootropic for cognitive research. Complementary to EPO protocols investigating neurological aspects of performance optimization.
- Selank 11mg – Anxiolytic peptide for stress research. Combined with EPO in protocols examining psychological aspects of performance enhancement.
- Cerebrolysin 60mg – Neurotrophic peptide for brain health. Research investigating EPO’s neuroprotective effects alongside dedicated neurotrophic agents.
- Pinealon 5mg – Brain-specific peptide for neuroprotection. Complementary to EPO protocols investigating central nervous system effects.
Tissue Repair and Recovery
- MGF 2mg – Mechano Growth Factor for muscle-specific research. Complementary to EPO protocols investigating muscle adaptations to enhanced oxygen delivery.
- Follistatin 1mg – Myostatin inhibitor for muscle growth research. Combined protocols examine anabolic effects alongside EPO’s aerobic benefits.
Anti-Aging and Longevity
- Epitalon 10mg – Telomerase activator for longevity research. Complementary to EPO protocols investigating aging effects on erythropoiesis and performance.
- Thymalin 10mg – Thymus peptide for immune research. Combined protocols investigate immune-hematological interactions during EPO treatment.
- Thymosin Alpha-1 5mg – Immune modulator for comprehensive health research. Stacking with EPO examines immune system effects on erythropoiesis.
Fertility and Reproductive Research
- Kisspeptin-10 5mg – HPG axis regulator for fertility research. Investigates hormonal regulation of EPO production and erythropoiesis.
- Oxytocin 2mg – Social bonding peptide for behavioral research. Complementary to EPO protocols investigating psychological aspects of performance.
Aesthetic and Skin Research
- Melanotan-1 10mg – FDA-approved melanocortin agonist. Shares receptor family with EPO, enabling comparative signaling studies.
- Melanotan 2 10mg – Multi-receptor melanocortin agonist. Research investigating melanocortin system interactions with erythropoiesis.
- PT-141 10mg – Bremelanotide for sexual function research. Complementary to EPO protocols investigating comprehensive performance optimization.
- Snap-8 10mg – Anti-wrinkle peptide for aesthetic research. Complementary to EPO protocols investigating overall health optimization.
Immune and Inflammation Research
- Glutathione 1500mg – Master antioxidant for oxidative stress research. Stacking with EPO investigates antioxidant protection during increased oxygen transport.
Essential Research Supplies
- Bacteriostatic Water 3mL – Essential for EPO 3000IU reconstitution. Each vial requires 1.0 mL bacteriostatic water to create 3000 IU/mL concentration. Contains 0.9% benzyl alcohol preservative.
- Peptide Calculator – Free online tool for calculating precise peptide doses, reconstitution volumes, and injection amounts. Essential for accurate EPO 3000IU dosing in research protocols.
- Shop Peptides – Complete peptide catalog including all performance peptides, hormones, and specialty research compounds.
Customer Support
- Contact Us – Technical support for EPO 3000IU research questions, protocol design assistance, and product information.
- Research Resources – Educational materials, published studies, and research protocols for EPO and related performance research.
Buy HMG peptide for fertility and testosterone research with access to these comprehensive related products and resources. PrymaLab offers the complete range of peptides and supplies needed for advanced reproductive endocrinology research, all backed by rigorous quality control and expert technical support.
Compliance and Legal Disclaimer
IMPORTANT: RESEARCH USE ONLY
Buy HMG peptide for fertility and testosterone research with complete understanding of its intended use and legal status. Human Menopausal Gonadotropin (HMG) 75IU is supplied by PrymaLab exclusively for research purposes and is not intended for human consumption, medical treatment, or clinical use.
Research Use Declaration
This product is intended solely for:
- In vitro research applications
- Laboratory investigations
- Scientific studies
- Educational purposes
- Non-clinical research protocols
NOT FOR HUMAN CONSUMPTION
HMG 75IU is NOT:
- A medication or pharmaceutical drug
- Intended for human consumption or administration
- Approved by the FDA for medical treatment
- A substitute for medical care or prescription medications
- Intended to diagnose, treat, cure, or prevent any disease
Regulatory Status
- This product has not been evaluated by the Food and Drug Administration (FDA)
- Not approved for medical use in humans
- Supplied for research purposes only under applicable regulations
- Researchers are responsible for compliance with local, state, and federal regulations
- Institutional review board (IRB) approval may be required for certain research applications
Age Restrictions
- Must be 18 years of age or older to purchase
- Intended for use by qualified researchers and scientific professionals
- Not intended for use by minors under any circumstances
Professional Use Only
HMG 75IU should only be used by:
- Qualified researchers with appropriate training
- Scientific professionals in laboratory settings
- Individuals with knowledge of peptide handling and research protocols
- Those operating under proper institutional oversight
No Medical Claims
PrymaLab makes no claims regarding:
- Medical efficacy or therapeutic benefits
- Treatment of any medical condition
- Diagnosis or prevention of disease
- Health outcomes or clinical results
Any information provided is for educational and research purposes only and should not be construed as medical advice.
Liability Disclaimer
- PrymaLab is not responsible for misuse of this product
- Users assume all risks associated with research applications
- No warranty is provided for outcomes or results
- PrymaLab is not liable for any adverse effects from improper use
- Researchers are responsible for following proper safety protocols
Intellectual Property
- Product information is provided for educational purposes
- Research findings and protocols remain the property of the researcher
- PrymaLab respects intellectual property rights of all parties
- Proper citation of sources is encouraged in published research
International Shipping
- Researchers are responsible for compliance with import regulations in their country
- Some countries may restrict or prohibit importation of research peptides
- Customs clearance is the responsibility of the purchaser
- PrymaLab is not responsible for seized or delayed shipments due to customs issues
Proper Disposal
- Dispose of unused product according to local regulations for biohazardous waste
- Follow institutional guidelines for peptide disposal
- Do not dispose in regular household trash or sewage systems
- Used syringes must be disposed in approved sharps containers
Ethical Research Practices
Researchers using HMG 75IU are expected to:
- Follow ethical research guidelines and principles
- Obtain necessary approvals from institutional review boards
- Maintain proper documentation and records
- Report adverse events or safety concerns
- Respect human and animal welfare in research applications
Product Quality Commitment
While HMG 75IU is for research use only, PrymaLab maintains:
- Pharmaceutical-grade manufacturing standards
- Rigorous quality control testing
- Third-party verification of purity and potency
- Complete documentation and traceability
- Commitment to consistent product quality
Consultation Recommendation
Before initiating any research protocol involving HMG 75IU:
- Consult with qualified medical or scientific professionals
- Review relevant literature and published research
- Ensure proper training in peptide handling and administration
- Obtain necessary institutional approvals
- Establish appropriate monitoring and safety protocols
Changes to Terms
PrymaLab reserves the right to:
- Modify product specifications as needed
- Update compliance requirements based on regulatory changes
- Discontinue products or change availability
- Revise terms and conditions of sale
Contact Information
For questions regarding compliance, regulatory status, or proper use:
Acknowledgment
By purchasing HMG 75IU from PrymaLab, you acknowledge that:
- You have read and understood this disclaimer
- You are 18 years of age or older
- You are a qualified researcher or scientific professional
- You will use this product for research purposes only
- You will not use this product for human consumption
- You accept full responsibility for proper and legal use
- You will comply with all applicable regulations and laws
Buy HMG peptide for fertility and testosterone research with full understanding of these compliance requirements and legal limitations. PrymaLab is committed to supporting legitimate scientific research while ensuring products are used appropriately and legally.

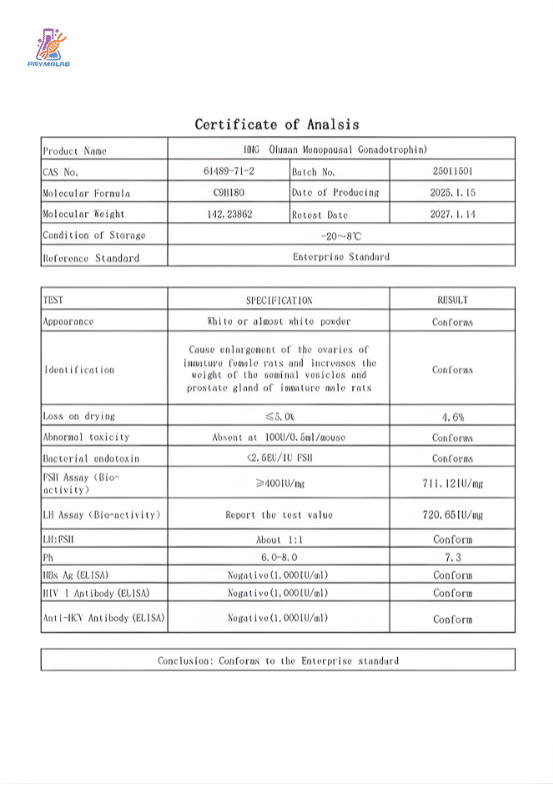






Reviews
There are no reviews yet.