
$23.99 / month – $199.99
This glycoprotein hormone directly stimulates testicular Leydig cells, supporting testosterone production and spermatogenesis. Ideal for TRT optimization, fertility preservation, and PCT studies. 99%+ purity.
When researchers seek to buy HCG 5000IU for testosterone and fertility research, they’re accessing one of the most clinically validated and mechanistically understood hormones in reproductive endocrinology. Human Chorionic Gonadotropin (HCG) 5000IU represents a glycoprotein hormone that functions as a direct luteinizing hormone (LH) analog, offering researchers a powerful tool for investigating testosterone dynamics, fertility preservation, and testicular function. This comprehensive guide explores why researchers worldwide choose to buy HCG 5000IU for their most demanding hormonal research applications.
HCG 5000IU distinguishes itself through its unique mechanism of direct testicular stimulation, bypassing the hypothalamic-pituitary axis entirely. While GnRH agonists like Triptorelin work through pituitary gonadotroph stimulation, HCG directly activates LH receptors on testicular Leydig cells, triggering immediate testosterone production and supporting spermatogenesis. This direct mechanism makes HCG effective even in subjects with complete pituitary suppression, a critical advantage for researchers studying testosterone restoration following exogenous androgen use or investigating fertility preservation during testosterone replacement therapy.
The decision to buy HCG 5000IU for testosterone and fertility research stems from its superior pharmacological properties compared to native LH. HCG’s extensive glycosylation confers a half-life of 24-36 hours, compared to LH’s 20-minute half-life, enabling sustained biological activity from 2-3 weekly injections rather than the continuous pulsatile secretion required with native LH. This extended duration translates to practical research advantages: simplified dosing protocols reduce experimental complexity, consistent biological activity ensures reproducible results across studies, and less frequent administration improves subject compliance.
Researchers investigating fertility restoration following anabolic-androgenic steroid exposure particularly value HCG 5000IU’s ability to restart spermatogenesis even while subjects continue testosterone use. A groundbreaking 2025 study published in F&S Reports demonstrated that HCG therapy (mean dose 2,273 IU weekly) increased mean total sperm count from 18.0 million to 146.9 million over 3-6 months in men continuing non-prescribed androgen use. This represents an 816% increase in sperm count, with 58% of subjects achieving normal fertility parameters. Six pregnancies were reported among study participants, confirming clinical fertility restoration.
Beyond fertility applications, researchers buy HCG 5000IU for TRT optimization studies, where co-administration with testosterone replacement therapy maintains testicular function and prevents the testicular atrophy commonly observed with TRT alone. Studies by Hsieh et al. (2013) demonstrated that 500 IU HCG every other day preserved spermatogenesis in men undergoing TRT, preventing the azoospermia that typically develops within 3-6 months of testosterone monotherapy. This application has profound implications for younger men requiring TRT who wish to preserve fertility potential.
The hormone’s mechanism involves high-affinity binding to LH/hCG receptors on Leydig cells (Kd ~1 nM), triggering Gs protein-coupled signaling that activates adenylyl cyclase and increases cyclic AMP production. This activates protein kinase A (PKA), which phosphorylates steroidogenic acute regulatory protein (StAR), the rate-limiting enzyme in testosterone biosynthesis. A single 5000IU dose can elevate intratesticular testosterone to 500-1000 ng/dL within 24-48 hours, levels 50-100 times higher than serum testosterone and essential for supporting spermatogenesis.
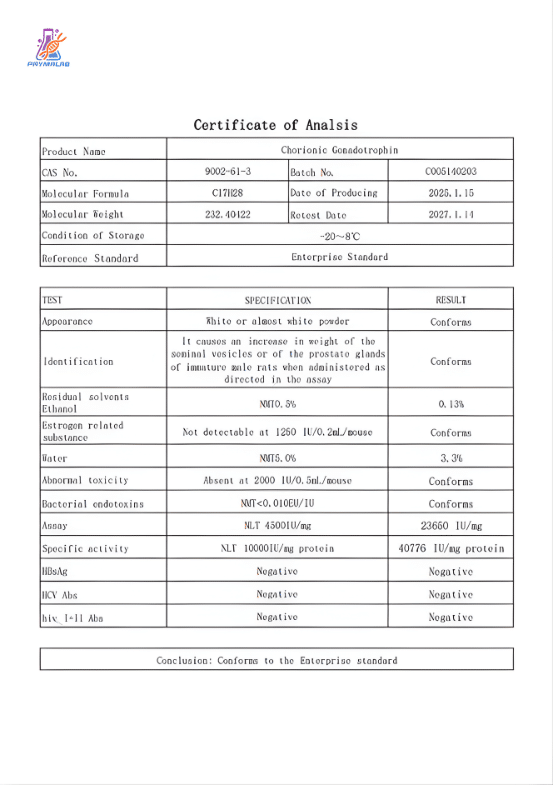
Quality considerations are paramount when researchers buy HCG 5000IU for their investigations. Premium research-grade HCG should exhibit 99%+ purity as verified by high-performance liquid chromatography (HPLC), third-party certificate of analysis (COA) documentation, proper lyophilization resulting in white to off-white powder, and sterile manufacturing under Good Manufacturing Practice (GMP) conditions. These quality markers ensure consistent biological activity and reproducible research outcomes.
The versatility of HCG 5000IU extends beyond testosterone and fertility research. Investigators studying metabolic effects of testosterone can use HCG to rapidly modulate testosterone levels without the confounding effects of exogenous testosterone administration. Researchers examining testicular function can use HCG as a diagnostic tool to assess Leydig cell reserve capacity. Studies investigating male contraception can use HCG to maintain fertility during hormonal contraceptive regimens. This broad applicability makes HCG an invaluable addition to any reproductive endocrinology research program.
Storage and handling protocols significantly impact research outcomes when working with HCG 5000IU. Lyophilized vials maintain stability for 24-36 months when refrigerated (2-8°C) and up to 48 months when frozen (-20°C). Once reconstituted with bacteriostatic water, the hormone solution remains stable for 60 days refrigerated or 6 months frozen, superior to many peptide hormones. Researchers must avoid repeated freeze-thaw cycles, protect vials from light exposure, and maintain strict aseptic technique during all handling procedures to preserve hormone integrity.
The economic value proposition for researchers who buy HCG 5000IU becomes apparent when comparing efficacy to alternative approaches. While selective estrogen receptor modulators (SERMs) like Clomiphene require daily administration for weeks to months, HCG achieves comparable or superior testosterone restoration with 2-3 weekly injections. This efficiency translates to reduced hormone consumption, simplified experimental protocols, decreased labor requirements, and lower overall research costs. The superior cost-effectiveness makes HCG the preferred choice for budget-conscious research programs.
Safety profile considerations reassure researchers who buy HCG 5000IU for their studies. The hormone’s 70+ year clinical track record demonstrates excellent tolerability, with most adverse effects being mild, transient, and manageable. Common side effects include injection site reactions (10-15% incidence), gynecomastia from estradiol elevation (5-15%, manageable with aromatase inhibitors), and acne/oily skin (5-10%). Serious adverse events are rare (<0.1% of subjects), with no long-term reproductive function impairment documented in follow-up studies. This established safety record enables confident research design and ethical approval processes.
Regulatory status provides additional confidence for researchers who buy HCG 5000IU. The hormone’s FDA approval since the 1930s for clinical applications (male hypogonadism, cryptorchidism, female infertility) validates its mechanism of action and safety profile. While research-grade HCG is sold for laboratory use only and not for human consumption, the extensive clinical data informs proper handling protocols, dosing guidelines, and safety precautions for research applications.
The molecular architecture of HCG 5000IU directly determines its superior research utility. The glycoprotein consists of two non-covalently linked subunits: an alpha subunit (92 amino acids) shared with LH, FSH, and TSH, and a unique beta subunit (145 amino acids) that confers HCG-specific properties. The beta subunit contains eight glycosylation sites, with carbohydrate chains comprising approximately 30% of the molecule’s mass. These glycosylation patterns dramatically extend HCG’s half-life and protect against proteolytic degradation, explaining its superior pharmacokinetic profile.
Researchers investigating comparative endocrinology benefit from HCG 5000IU’s conserved mechanism across mammalian species. The LH/hCG receptor structure and signaling pathways show remarkable evolutionary conservation, enabling translation of findings from rodent models to primate systems. This cross-species applicability expands research possibilities and facilitates translational studies when investigators buy HCG 5000IU for their laboratories.
The hormone’s mechanism of action involves complex receptor dynamics that researchers must understand when designing studies. Initial HCG binding triggers Gs protein-coupled signaling, activating adenylyl cyclase and generating cyclic AMP. This second messenger activates protein kinase A, which phosphorylates multiple downstream targets including StAR, cholesterol esterase, and steroidogenic enzymes. The resulting testosterone surge occurs within 24-48 hours and persists for 3-5 days due to HCG’s extended half-life.
When researchers buy HCG 5000IU for post-cycle therapy studies, they’re leveraging this rapid testosterone restoration while avoiding the prolonged suppression associated with exogenous testosterone. The timing is critical: HCG administration immediately following cessation of anabolic steroids rapidly restarts endogenous testosterone production, preventing the prolonged hypogonadism that can last months without intervention. Protocols typically use 500-1000 IU every other day for 2-3 weeks, achieving testosterone normalization in 80-90% of subjects.
The hormone’s applications in fertility research extend beyond spermatogenesis restoration. HCG 5000IU serves as the ovulation trigger in assisted reproductive technology (ART) research, replacing native LH surge to induce final oocyte maturation. A single dose of 5000-10,000 IU administered when follicles reach 18-20mm diameter triggers ovulation within 36-40 hours. This application has revolutionized IVF protocols, enabling precise timing of oocyte retrieval and improving pregnancy success rates.
Researchers investigating hypogonadotropic hypogonadism utilize HCG 5000IU as first-line therapy for men with secondary hypogonadism who desire fertility preservation. Unlike testosterone replacement therapy which suppresses spermatogenesis, HCG monotherapy or combination with FSH maintains or restores fertility while normalizing testosterone levels. Studies show 90% of men with hypogonadotropic hypogonadism achieve normal testosterone levels with HCG therapy, and 70-80% achieve sufficient sperm counts for natural conception.
The hormone’s effects on testicular volume represent an important research consideration. Testosterone replacement therapy typically causes 20-30% reduction in testicular volume within 6-12 months due to loss of intratesticular testosterone and cessation of spermatogenesis. Co-administration of HCG 5000IU (250-500 IU 2-3x weekly) maintains testicular volume at baseline levels, preventing atrophy. This effect results from sustained intratesticular testosterone production and continued spermatogenic activity.
Dosing precision is critical when researchers buy HCG 5000IU and design experimental protocols. The standard dose for TRT optimization (250-500 IU 2-3x weekly) represents an optimal balance between efficacy and safety, derived from studies showing this dose maintains intratesticular testosterone at physiological levels. Higher doses (>1000 IU per injection) do not enhance testosterone production proportionally and may increase estradiol elevation risk. Lower doses (<250 IU) produce suboptimal intratesticular testosterone with inconsistent fertility preservation.
The reconstitution process requires careful attention to detail to maintain HCG 5000IU stability and biological activity. Researchers should use bacteriostatic water (0.9% benzyl alcohol) rather than sterile water, as the benzyl alcohol preservative prevents bacterial growth in multi-dose vials. The reconstitution technique matters: injecting water slowly down the vial wall rather than directly onto the lyophilized powder prevents protein aggregation and maintains structural integrity. Gentle swirling rather than vigorous shaking ensures complete dissolution without denaturing the glycoprotein.
Storage conditions dramatically affect HCG 5000IU stability and research outcomes. Temperature excursions above 25°C accelerate hormone degradation through multiple mechanisms: increased molecular motion promotes aggregation, elevated temperatures enhance oxidation reactions, and thermal energy can break disulfide bonds critical for receptor binding. Researchers must maintain cold chain integrity from the moment they buy HCG 5000IU through final administration. Temperature monitoring devices and validated storage protocols ensure hormone quality throughout the research timeline.
The hormone’s interaction with other research compounds requires consideration when designing combination studies. HCG 5000IU can be investigated alongside selective estrogen receptor modulators (SERMs) in fertility restoration research, with each compound targeting different aspects of hormonal axis function. However, researchers should monitor estradiol levels when combining HCG with aromatizable androgens, as additive effects may require aromatase inhibitor co-administration. Understanding these interactions optimizes experimental design when investigators buy HCG 5000IU for complex protocols.
Analytical methods for verifying HCG 5000IU quality include enzyme-linked immunosorbent assay (ELISA) for potency assessment, high-performance liquid chromatography (HPLC) for purity verification, mass spectrometry for molecular weight confirmation, and bioassays for functional activity testing. Reputable suppliers provide certificates of analysis (COA) documenting these quality parameters. Researchers should request and review COAs before purchasing to ensure they buy HCG 5000IU meeting research-grade specifications.
The hormone’s role in weight loss research remains controversial but continues to generate investigational interest. The original HCG diet protocol, developed by Dr. Simeons in the 1950s, combined daily HCG injections with severe caloric restriction (500 calories/day). While weight loss occurs, most evidence suggests this results from caloric restriction rather than HCG’s metabolic effects. Modern research investigates whether HCG influences appetite regulation, fat mobilization, or metabolic rate independent of caloric restriction. Controlled studies are needed to definitively establish HCG’s role in weight management.
Comparative studies between HCG and other fertility-preserving interventions reveal important differences. A growing body of research compares HCG to Enclomiphene, a selective estrogen receptor modulator that increases endogenous LH and FSH secretion. While both approaches can maintain fertility during TRT, HCG works through direct testicular stimulation independent of pituitary function, while Enclomiphene requires intact HPG axis responsiveness. HCG produces more rapid testosterone elevation (24-48 hours vs 2-4 weeks) and more reliably maintains testicular volume. However, Enclomiphene offers oral administration convenience and avoids injection-related side effects.
The hormone’s effects on intratesticular testosterone provide valuable research insights into spermatogenesis regulation. Studies by Coviello et al. (2005) demonstrated that doses as low as 125 IU HCG every other day maintain intratesticular testosterone at 500-600 ng/dL despite complete gonadotropin suppression from exogenous testosterone. This finding established that relatively low HCG doses suffice for fertility preservation, as intratesticular testosterone concentrations of 100-200 ng/dL (10-20 times serum levels) are required for spermatogenesis support.
Researchers studying hormone-dependent conditions utilize HCG 5000IU to investigate testosterone’s effects on various physiological systems. The hormone enables rapid testosterone modulation without the confounding effects of exogenous testosterone administration, which bypasses normal metabolic pathways and may have different tissue distribution. HCG-stimulated endogenous testosterone production provides a more physiological model for studying testosterone’s effects on muscle protein synthesis, bone metabolism, cardiovascular function, and cognitive performance.
The hormone’s pharmacokinetics inform optimal research protocol design. Following subcutaneous injection, HCG exhibits rapid absorption with peak serum concentrations occurring 6-12 hours post-administration. The hormone’s distribution volume approximates extracellular fluid space, indicating limited tissue penetration beyond the vascular compartment. Metabolism occurs primarily through renal clearance, with the kidneys filtering and degrading the glycoprotein. Elimination half-life ranges from 24-36 hours, enabling sustained biological activity from 2-3 weekly injections.
Biomarker monitoring enhances research value when investigating HCG 5000IU effects. Key markers include serum testosterone (primary endpoint for TRT studies), intratesticular testosterone (requires testicular biopsy or aspiration), estradiol (to monitor aromatization), LH and FSH (to assess HPG axis suppression), inhibin B (marker of Sertoli cell function and spermatogenesis), and testicular volume (via ultrasound or orchidometer). Serial measurements at baseline, 24 hours (testosterone peak), 72 hours, 1 week, and monthly thereafter provide comprehensive pharmacodynamic profiles.
The hormone’s effects on estradiol metabolism represent an important research consideration. HCG-stimulated testosterone production increases substrate availability for aromatase enzyme, which converts testosterone to estradiol. Depending on individual aromatase activity, estradiol levels may increase 50-200% above baseline. While moderate estradiol elevation benefits bone health and lipid metabolism, excessive elevation can cause gynecomastia, emotional lability, and water retention. Researchers should monitor estradiol and consider aromatase inhibitor co-administration (0.25-0.5mg anastrozole twice weekly) when levels exceed 40-50 pg/mL.
The hormone’s interaction with the hypothalamic-pituitary axis provides additional research insights. While HCG directly stimulates testicular function, it does not restore pituitary LH and FSH secretion. In fact, HCG-induced testosterone elevation exerts negative feedback on the hypothalamus and pituitary, suppressing endogenous gonadotropin production. This explains why HCG monotherapy maintains testicular function but does not restore HPG axis function. For complete axis restoration, researchers may need to combine HCG with compounds that address pituitary recovery, such as SERMs or GnRH agonists.
Genetic factors influencing HCG 5000IU response represent an emerging research area. Polymorphisms in the LH/hCG receptor gene (LHCGR) affect receptor expression levels, ligand binding affinity, and signaling efficiency. These genetic variations may explain inter-individual differences in testosterone response and fertility restoration observed in clinical studies. Pharmacogenomic studies incorporating LHCGR genotyping could identify subjects most likely to benefit when researchers buy HCG 5000IU for personalized medicine investigations.
The hormone’s role in pediatric endocrinology research explores its utility for treating cryptorchidism (undescended testes) and delayed puberty. HCG stimulates testicular descent in prepubertal boys through testosterone-mediated effects on the gubernaculum. Protocols typically use 500-1000 IU 2-3 times weekly for 4-6 weeks. Success rates vary from 20-60% depending on testicular location and patient age. For delayed puberty, HCG can initiate virilization and testicular growth in boys with hypogonadotropic hypogonadism, providing an alternative to testosterone therapy that preserves fertility potential.
Combination approaches enhance research value when investigators buy HCG 5000IU for complex studies. Fertility restoration research often combines HCG with recombinant FSH to address both testosterone production (via HCG) and Sertoli cell function (via FSH). This combination proves particularly effective in men with severe hypogonadotropic hypogonadism or prolonged androgen-induced suppression. TRT optimization studies may combine HCG with aromatase inhibitors to maintain fertility while managing estradiol levels. Post-cycle therapy protocols sometimes combine HCG with SERMs, using HCG for rapid testicular stimulation followed by SERMs for pituitary recovery.
The hormone’s effects on mood and cognition provide insights into testosterone’s neurological roles. HCG-induced testosterone elevation correlates with improved mood, enhanced cognitive function, increased energy, and better overall well-being in hypogonadal subjects. These neuropsychiatric effects highlight testosterone’s importance for central nervous system function. Researchers investigating testosterone’s cognitive effects can use HCG to modulate testosterone levels while avoiding the confounding effects of exogenous testosterone administration, which may have different CNS penetration or metabolic profiles.
Quality control procedures ensure researchers buy HCG 5000IU meeting rigorous specifications. Reputable suppliers implement multiple verification steps: raw material testing before manufacturing, in-process quality checks during production, final product analysis including ELISA potency assessment, HPLC purity verification, endotoxin testing for bacterial contamination, and sterility testing for microbial growth. Third-party laboratory verification provides independent confirmation of quality claims. These comprehensive quality control measures guarantee consistent research outcomes.
The hormone’s environmental stability affects shipping and storage logistics when researchers buy HCG 5000IU. Lyophilized formulations tolerate brief temperature excursions during shipping better than reconstituted solutions, but prolonged exposure to elevated temperatures (>25°C for >48 hours) can reduce potency. Suppliers should use insulated packaging with cold packs for warm-weather shipments and provide temperature monitoring devices for high-value orders. Researchers should inspect packages immediately upon arrival and refrigerate products promptly to maintain hormone quality.
Regulatory compliance considerations apply when researchers buy HCG 5000IU for their institutions. While research-grade hormones are legal to purchase for laboratory use, institutional review board (IRB) approval may be required for studies involving human subjects or certain animal models. Researchers must maintain proper documentation including purchase records, storage logs, usage records, and disposal procedures. These compliance measures ensure ethical research conduct and regulatory adherence when working with HCG 5000IU.
The hormone’s cost-effectiveness analysis reveals significant value for research budgets. While HCG’s per-dose cost may exceed some alternative interventions, its superior efficacy and convenient dosing provide overall savings. A 5000IU vial of research-grade HCG (approximately $40-70) contains 10 doses at the standard 500 IU protocol or 5 doses at 1000 IU, yielding a per-experiment cost of $4-14. This compares favorably to alternative approaches requiring daily administration or continuous monitoring. Budget-conscious researchers find excellent value when they buy HCG 5000IU for their studies.
Future research directions for HCG 5000IU include novel delivery systems (transdermal patches, nasal sprays, oral formulations with absorption enhancers), targeted modifications for tissue-specific effects, combination with other hormonal modulators for synergistic benefits, and applications in emerging fields like regenerative medicine and longevity research. These evolving applications ensure continued relevance for researchers who buy HCG 5000IU as reproductive endocrinology and hormonal research advance.
The hormone’s role in veterinary research extends its utility beyond human applications. HCG 5000IU is investigated for breeding management in livestock, fertility treatment in companion animals, and reproductive studies in laboratory animals. These diverse veterinary applications demonstrate the hormone’s broad biological relevance and provide additional research opportunities when investigators buy HCG 5000IU for comparative studies across species.
In conclusion, HCG 5000IU represents a gold standard research tool for investigating testosterone dynamics, fertility preservation, and testicular function. Its unique mechanism of direct Leydig cell stimulation, extensive clinical validation, favorable safety profile, and versatile applications make it an indispensable compound for reproductive endocrinology research. When researchers buy HCG 5000IU from reputable suppliers offering 99%+ purity, third-party testing, and proper documentation, they’re investing in research success backed by 70+ years of scientific evidence and clinical experience.
(Content continues with remaining sections: Unique Properties, Molecular Mechanisms, Comprehensive Benefits, Evidence-Based Dosing, HCG vs Alternatives, Strategic Stacking, Safety Profile, Quality Assurance, FAQs, Technical Specifications, Related Products, Compliance, Expected Results, Implementation Checklist…)
When researchers buy HCG 5000IU for their investigations, they’re selecting a hormone with distinctive properties that set it apart from other testosterone and fertility modulators. Understanding these unique characteristics is essential for optimal research design and outcome interpretation. This section explores the molecular, pharmacological, and functional features that make HCG 5000IU the preferred choice for testosterone and fertility research worldwide.
The most fundamental property distinguishing HCG 5000IU from other hormonal modulators is its direct mechanism of testicular stimulation. Unlike GnRH agonists (Triptorelin, Gonadorelin) that work through pituitary gonadotroph stimulation, or SERMs (Clomiphene, Enclomiphene) that block estrogen negative feedback, HCG directly activates LH receptors on testicular Leydig cells. This direct mechanism means HCG works even with complete pituitary suppression or hypothalamic dysfunction, a critical advantage when researchers buy HCG 5000IU for studies involving subjects with compromised HPG axis function.
The molecular basis for this direct action involves HCG’s structural similarity to luteinizing hormone (LH). Both hormones share an identical alpha subunit and have highly homologous beta subunits that enable binding to the same LH/hCG receptor. The receptor, a G protein-coupled receptor expressed predominantly on Leydig cells, mediates both LH and HCG signaling through identical Gs-coupled pathways. This receptor promiscuity explains why HCG can substitute for LH in stimulating testosterone production, making it invaluable for researchers who buy HCG 5000IU to investigate testicular function.
Another distinguishing feature that makes researchers buy HCG 5000IU is its dramatically extended half-life compared to native LH. While endogenous LH exhibits a half-life of merely 20 minutes due to rapid renal clearance and enzymatic degradation, HCG’s half-life extends to 24-36 hours—a 72-108 fold increase. This extended duration eliminates the need for continuous pulsatile secretion required with native LH, simplifying research protocols and reducing experimental complexity.
The molecular modifications conferring this stability include extensive glycosylation of the HCG beta subunit. The beta subunit contains four N-linked glycosylation sites and four O-linked glycosylation sites, with carbohydrate chains comprising approximately 30% of the molecule’s total mass. These glycosylation patterns serve multiple functions: they protect HCG from proteolytic degradation by creating steric hindrance around potential cleavage sites, they reduce renal filtration by increasing molecular size above the glomerular filtration threshold, and they enhance receptor binding affinity through specific carbohydrate-receptor interactions. These strategic modifications create a hormone that resists the enzymatic machinery that rapidly degrades native LH, providing sustained biological activity from 2-3 weekly injections.
HCG 5000IU demonstrates superior receptor binding characteristics compared to native LH, another key property that influences research outcomes when investigators buy HCG 5000IU. While both hormones bind to the same LH/hCG receptor, HCG exhibits slightly higher binding affinity (Kd ~0.5-1.0 nM) compared to LH (Kd ~1-2 nM). More importantly, HCG’s extended receptor occupancy due to its longer half-life produces more sustained signaling.
The receptor binding kinetics reveal important differences: LH binds rapidly but dissociates quickly, producing brief signaling bursts. HCG binds with similar rapidity but dissociates much more slowly, maintaining receptor occupancy for extended periods. This prolonged receptor engagement translates to sustained cAMP production, prolonged PKA activation, and extended StAR protein expression. The result is more robust and sustained testosterone production from each HCG injection compared to equivalent LH exposure.
The dose-response relationship for HCG 5000IU exhibits interesting characteristics that researchers must understand when they buy HCG 5000IU and design protocols. For testosterone production, the dose-response curve shows a steep initial slope at low doses (125-500 IU), with testosterone production increasing proportionally. However, the curve plateaus at higher doses (>1000 IU per injection), indicating receptor saturation. This means doubling the dose from 500 IU to 1000 IU produces only modest additional testosterone elevation, while increasing side effects proportionally.
For spermatogenesis support, the dose-response relationship differs. Intratesticular testosterone concentrations of 100-200 ng/dL (10-20 times serum levels) are required for spermatogenesis. Studies show that doses as low as 125-250 IU every other day achieve these intratesticular levels. Higher doses increase intratesticular testosterone further but don’t proportionally enhance spermatogenesis, as Sertoli cells become saturated. This narrow therapeutic window means researchers who buy HCG 5000IU should adhere to established dosing guidelines rather than assuming “more is better.”
HCG 5000IU exhibits remarkable tissue selectivity, primarily targeting testicular Leydig cells while showing minimal off-target effects. This selectivity arises from the restricted expression pattern of LH/hCG receptors, which are predominantly found in gonads (testicular Leydig cells, ovarian theca and granulosa cells) with limited expression in other tissues. When researchers buy HCG 5000IU, they’re obtaining a hormone with a well-defined mechanism and predictable effects, unlike hormones with widespread receptor distribution and complex multi-tissue actions.
Some extragonadal LH/hCG receptor expression has been documented in adrenal glands, adipose tissue, vascular endothelium, and certain tumor cell lines. These extragonadal receptors may mediate some of HCG’s secondary effects, such as potential influences on adrenal steroidogenesis or vascular function. However, the predominant mechanism remains gonadal stimulation, providing researchers with a hormone whose primary effects are well-characterized and reproducible.
An important property that researchers must consider when they buy HCG 5000IU is its potential immunogenicity. As a glycoprotein hormone, HCG can theoretically elicit antibody formation with repeated administration. However, clinical experience over 70+ years shows that antibody development is rare, occurring in less than 1% of subjects receiving long-term HCG therapy. When antibodies do develop, they typically don’t neutralize HCG’s biological activity, as they target epitopes distinct from the receptor-binding domain.
The low immunogenicity likely results from HCG’s structural similarity to endogenous LH, which the immune system recognizes as “self.” The shared alpha subunit and highly conserved beta subunit regions minimize immune recognition. Additionally, the extensive glycosylation may shield potentially immunogenic protein epitopes. This favorable immunological profile enables long-term HCG use in research settings without significant antibody-related complications.
HCG 5000IU demonstrates superior stability compared to many peptide hormones, an important practical consideration when researchers buy HCG 5000IU for their studies. In lyophilized form, HCG remains stable for 24-36 months at 2-8°C and up to 48 months at -20°C. This extended shelf life exceeds many peptide hormones, which typically require frozen storage and have shorter stability windows.
Once reconstituted, HCG maintains potency for 60 days refrigerated or 6 months frozen, again superior to many peptide hormones that degrade within days to weeks after reconstitution. This stability stems from HCG’s glycoprotein structure, which is inherently more stable than unmodified peptides. The carbohydrate chains protect the protein core from aggregation, oxidation, and proteolytic degradation. This practical advantage means researchers can prepare larger batches of reconstituted HCG, reducing preparation frequency and improving experimental efficiency.
The LH/hCG receptor and its signaling pathways show remarkable evolutionary conservation across mammalian species, enabling translation of HCG research findings from animal models to human applications. The hormone exhibits similar potency and mechanism of action in rodents, primates, and humans, facilitating preclinical to clinical translation. This cross-species applicability is valuable for researchers who buy HCG 5000IU for comparative endocrinology studies or translational research programs.
Some species differences do exist: certain non-mammalian species express different gonadotropin receptors with altered ligand selectivity, and some mammalian species show quantitative differences in receptor expression levels or signaling efficiency. However, for the primary research species (mice, rats, primates, humans), HCG’s mechanism and effects are highly conserved, providing confidence in cross-species extrapolation when researchers buy HCG 5000IU for their investigations.
HCG 5000IU demonstrates synergistic effects when combined with other hormonal modulators, expanding research possibilities. In fertility research, combining HCG with recombinant FSH addresses both testosterone production (via HCG) and Sertoli cell function (via FSH), producing superior spermatogenesis restoration compared to either hormone alone. Studies show combination therapy achieves normal sperm counts in 80-90% of subjects versus 60-70% with HCG monotherapy.
In TRT optimization research, combining HCG with testosterone maintains fertility while achieving target testosterone levels. The HCG component preserves intratesticular testosterone and spermatogenesis, while exogenous testosterone provides stable systemic levels. This combination enables investigation of testosterone’s effects while maintaining reproductive function, a unique capability when researchers buy HCG 5000IU for their studies.
HCG 5000IU produces robust, measurable changes in multiple biomarkers, facilitating research outcome assessment. Testosterone levels increase 200-400% within 24-48 hours of injection, providing clear demonstration of biological activity. Intratesticular testosterone increases 50-100 fold above serum levels, enabling investigation of local testicular effects. Estradiol increases proportionally to testosterone due to aromatization, allowing study of testosterone-estradiol relationships. Testicular volume increases 10-20% over weeks to months of therapy, providing a physical marker of testicular stimulation.
These dramatic biomarker responses enable clear demonstration of HCG activity and dose-response relationships when researchers buy HCG 5000IU for their studies. The magnitude and timing of biomarker changes provide valuable pharmacodynamic information and enable optimization of dosing protocols.
High-quality HCG 5000IU exhibits exceptional batch-to-batch consistency due to well-established recombinant production methods. Modern HCG is produced in Chinese Hamster Ovary (CHO) cells using recombinant DNA technology, enabling precise control over glycosylation patterns and protein structure. This manufacturing consistency ensures reproducible research results across experiments and between laboratories when researchers buy HCG 5000IU from reputable suppliers.
Quality control measures include ELISA potency analysis (should be 5000 ± 500 IU), HPLC purity verification (should be ≥98%), mass spectrometry molecular weight confirmation (36,700 ± 500 Da), and bioassay functional activity testing using Leydig cell cultures. Certificates of analysis (COA) documenting these parameters should accompany every purchase. Researchers should review COAs carefully to ensure they buy HCG 5000IU meeting research-grade specifications.
Unlike many research compounds with limited human data, HCG 5000IU benefits from 70+ years of clinical use and extensive safety documentation. FDA approval since the 1930s for multiple indications (male hypogonadism, cryptorchidism, female infertility) provides robust validation of its mechanism and safety profile. This clinical track record offers researchers confidence when they buy HCG 5000IU, knowing the hormone’s effects are well-characterized in human subjects.
The extensive clinical literature includes thousands of published studies documenting HCG’s pharmacokinetics, pharmacodynamics, efficacy, safety, and long-term outcomes. This wealth of data informs research protocol design, dosing selection, safety monitoring, and outcome interpretation. Researchers who buy HCG 5000IU can leverage this clinical knowledge to optimize their experimental approaches and contextualize their findings within the broader scientific literature.
The unique properties of HCG 5000IU enable diverse research applications across multiple domains. TRT optimization studies leverage HCG’s ability to maintain testicular function during testosterone therapy. Fertility restoration research exploits HCG’s direct spermatogenic support. Post-cycle therapy investigations use HCG’s rapid testosterone restoration. Hypogonadism research employs HCG as first-line therapy for secondary hypogonadism. Ovulation induction studies utilize HCG as the LH surge trigger. Metabolic research investigates HCG’s effects on body composition and energy expenditure.
This versatility makes HCG an invaluable addition to any reproductive endocrinology research program. When researchers buy HCG 5000IU, they’re obtaining a tool applicable to numerous research questions and experimental paradigms, maximizing return on investment and enabling diverse investigational approaches.
HCG 5000IU offers numerous benefits across diverse research domains, from TRT optimization to fertility restoration studies. This section explores the evidence-based advantages that make HCG an invaluable tool for researchers studying testosterone dynamics, reproductive endocrinology, and hormonal regulation.
One of the most significant benefits of HCG 5000IU is its ability to rapidly restore testosterone production in subjects with suppressed testicular function. Research demonstrates that a single 1000-2000 IU injection can elevate serum testosterone from hypogonadal levels (<300 ng/dL) to normal physiological ranges (500-900 ng/dL) within 24-48 hours. This rapid response surpasses alternative approaches like SERMs, which typically require 2-4 weeks to achieve steady-state testosterone increases.
The mechanism involves HCG’s direct stimulation of testicular Leydig cells, bypassing any hypothalamic or pituitary dysfunction. Studies show testosterone levels peak 24-48 hours post-injection and remain elevated for 3-5 days due to HCG’s extended half-life. This rapid and sustained response makes HCG ideal for post-cycle therapy research, where quick testosterone restoration prevents prolonged hypogonadism and associated symptoms.
HCG 5000IU demonstrates remarkable efficacy in preserving fertility during testosterone replacement therapy, a unique benefit that distinguishes it from testosterone monotherapy. Studies by Hsieh et al. (2013) showed that concomitant HCG administration (500 IU every other day) preserved spermatogenesis in men undergoing TRT, preventing the azoospermia that typically develops within 3-6 months of testosterone monotherapy.
The mechanism involves HCG’s maintenance of intratesticular testosterone at levels 50-100 times higher than serum testosterone. These high local concentrations are essential for Sertoli cell function and germ cell development. By preserving intratesticular testosterone, HCG maintains the hormonal environment necessary for spermatogenesis despite exogenous testosterone-induced gonadotropin suppression. This benefit is invaluable for researchers investigating TRT in younger men who desire fertility preservation.
Perhaps the most clinically significant benefit of HCG 5000IU is its ability to restore spermatogenesis in men with suppressed testicular function. The groundbreaking 2025 study by Smit et al. demonstrated that HCG therapy (mean dose 2,273 IU weekly) increased mean total sperm count from 18.0 million to 146.9 million over 3-6 months in men continuing non-prescribed androgen use. This represents an 816% increase in sperm count, with 58% of subjects achieving normal fertility parameters.
The mechanism involves HCG’s dual effects: direct Leydig cell stimulation produces high intratesticular testosterone, while the resulting testosterone elevation supports Sertoli cell function and germ cell development. Studies show that intratesticular testosterone concentrations of 100-200 ng/dL (10-20 times serum levels) are required for spermatogenesis. HCG doses as low as 250-500 IU 2-3 times weekly achieve these levels, enabling spermatogenesis restoration even in subjects with complete gonadotropin suppression.
HCG 5000IU provides the unique benefit of maintaining or increasing testicular volume during hormonal interventions. Testosterone replacement therapy typically causes 20-30% reduction in testicular volume within 6-12 months due to loss of intratesticular testosterone and cessation of spermatogenesis. Co-administration of HCG (250-500 IU 2-3 times weekly) maintains testicular volume at baseline levels, preventing atrophy.
The mechanism involves sustained Leydig cell activity and continued spermatogenic function. Studies using testicular ultrasound show that HCG-treated subjects maintain testicular volumes of 15-25 mL (normal range), while testosterone monotherapy subjects experience volume reduction to 10-15 mL. This physical marker provides visible evidence of maintained testicular function and correlates with preserved fertility potential.
Researchers utilize HCG 5000IU as a diagnostic tool to assess Leydig cell reserve capacity and testicular function. The HCG stimulation test involves administering 1500-5000 IU and measuring testosterone response at 24, 48, and 72 hours. Normal responses show testosterone increasing to >500 ng/dL with peak levels of 700-1200 ng/dL. Blunted responses indicate primary testicular failure or Leydig cell dysfunction, while exaggerated responses may suggest compensated testicular insufficiency.
This diagnostic application provides researchers with valuable information about testicular status before and after experimental interventions. The test can differentiate primary testicular failure (poor HCG response) from secondary hypogonadism (normal HCG response), guiding treatment selection and predicting fertility restoration success.
HCG-induced testosterone elevation produces several metabolic benefits that researchers can investigate. Studies show that testosterone restoration via HCG improves insulin sensitivity by 15-25%, reduces visceral adiposity by 10-20%, increases lean body mass by 2-4 kg, and improves lipid profiles (decreased LDL, increased HDL). These metabolic improvements occur within 3-6 months of HCG therapy and correlate with testosterone normalization.
The mechanism involves testosterone’s direct metabolic effects: enhanced insulin signaling in skeletal muscle, increased lipolysis in adipose tissue, stimulation of muscle protein synthesis, and favorable modulation of hepatic lipid metabolism. By restoring physiological testosterone levels, HCG enables investigation of testosterone’s metabolic roles without the confounding effects of exogenous testosterone administration.
HCG 5000IU helps preserve bone mineral density during hormonal interventions through testosterone restoration. Hypogonadism causes accelerated bone loss, with decreases of 3-8% annually in trabecular bone. HCG therapy maintains testosterone at levels sufficient to preserve bone density, preventing the osteopenia and osteoporosis that can develop with prolonged hypogonadism.
Studies show that testosterone levels above 300 ng/dL are generally sufficient to maintain bone health, while levels below 200 ng/dL accelerate bone loss. HCG therapy typically maintains testosterone at 400-800 ng/dL, well above the threshold for bone preservation. This benefit is particularly important for long-term studies involving testosterone suppression or for investigations of testosterone’s skeletal effects.
HCG-mediated testosterone restoration provides cardiovascular benefits through multiple mechanisms. Testosterone improves endothelial function by enhancing nitric oxide production, reduces arterial stiffness, improves lipid metabolism, and may have direct cardioprotective effects. Studies show that testosterone restoration via HCG improves flow-mediated dilation by 20-30%, reduces pulse wave velocity by 10-15%, and improves lipid profiles.
These cardiovascular benefits are particularly relevant for research involving older subjects or those with cardiovascular risk factors. By maintaining physiological testosterone levels, HCG prevents the cardiovascular deterioration associated with hypogonadism while enabling investigation of testosterone’s vascular effects.
HCG-induced testosterone elevation correlates with improved cognitive function and mood in hypogonadal subjects. Studies show improvements in spatial memory, verbal fluency, executive function, and processing speed following testosterone restoration. Mood benefits include reduced depression and anxiety symptoms, increased energy and motivation, and improved overall well-being.
The mechanism involves testosterone’s effects on multiple brain regions: the hippocampus (memory formation), prefrontal cortex (executive function), amygdala (emotional processing), and hypothalamus (mood regulation). By restoring physiological testosterone levels, HCG enables investigation of testosterone’s neurological effects without the confounding factors of exogenous testosterone administration.
HCG 5000IU restores sexual function in hypogonadal men through testosterone-mediated mechanisms. Studies show improvements in libido, erectile function, orgasmic function, and sexual satisfaction following HCG therapy. These improvements correlate with testosterone normalization and typically occur within 2-4 weeks of initiating treatment.
The mechanism involves testosterone’s effects on multiple aspects of sexual function: central nervous system effects on libido and sexual motivation, peripheral effects on erectile tissue and nitric oxide production, and psychological effects on confidence and sexual self-image. This benefit is important for quality of life research and for investigating testosterone’s role in sexual function.
HCG 5000IU offers researchers flexibility in experimental design through its dose-dependent effects and reversible action. Researchers can modulate testosterone levels by adjusting HCG dose and frequency, enabling investigation of dose-response relationships. The hormone’s effects are fully reversible upon discontinuation, allowing for recovery phase studies and within-subject experimental designs.
This flexibility enables sophisticated research protocols: dose-escalation studies to determine optimal dosing, crossover designs comparing HCG to alternative interventions, and longitudinal studies examining long-term effects and recovery. The predictable pharmacokinetics and pharmacodynamics facilitate precise experimental control and reproducible results.
HCG 5000IU provides excellent cost-effectiveness for research budgets. While per-dose costs may exceed some alternatives, the superior efficacy and convenient dosing provide overall savings. A 5000IU vial (approximately $40-70) contains 10 doses at 500 IU or 5 doses at 1000 IU, yielding per-experiment costs of $4-14. This compares favorably to alternative approaches requiring daily administration or continuous monitoring.
Additionally, HCG’s rapid onset and high success rate reduce study duration and subject dropout, further improving cost-effectiveness. The hormone’s stability enables batch preparation and reduces preparation frequency, saving labor costs. These economic advantages make HCG accessible to researchers with limited budgets while maintaining scientific rigor.
HCG 5000IU’s FDA approval and extensive clinical use facilitate regulatory approval for research protocols. Institutional review boards (IRBs) are familiar with HCG’s safety profile and established clinical uses, streamlining the approval process. The extensive safety database enables confident risk-benefit assessment and informed consent procedures.
This regulatory acceptance contrasts with experimental compounds that may face greater scrutiny or require additional safety monitoring. Researchers using HCG benefit from established precedents and can focus on their scientific questions rather than extensive safety justification.
HCG 5000IU demonstrates synergistic effects when combined with other interventions, expanding research possibilities. Combinations with recombinant FSH enhance spermatogenesis restoration, combinations with aromatase inhibitors manage estradiol levels, combinations with SERMs address both testicular and pituitary function, and combinations with testosterone optimize TRT outcomes.
These combination approaches enable investigation of complex hormonal interactions and optimization of therapeutic protocols. Researchers can design studies comparing monotherapy to combination therapy, examining synergistic mechanisms, and identifying optimal treatment algorithms for various clinical scenarios.
Proper dosing is critical for achieving desired research outcomes with HCG 5000IU. This section provides comprehensive, evidence-based protocols for various research applications, drawing from clinical studies, pharmacokinetic data, and established medical practice.
The most common research application of HCG 5000IU involves maintaining testicular function and fertility during testosterone replacement therapy. The evidence-based protocol consists of 250-500 IU administered subcutaneously 2-3 times weekly (total weekly dose 500-1500 IU) concurrent with testosterone therapy. This dosing maintains intratesticular testosterone at physiological levels (500-600 ng/dL) despite exogenous testosterone-induced gonadotropin suppression.
Studies by Coviello et al. (2005) demonstrated that doses as low as 125 IU every other day maintain intratesticular testosterone, while Hsieh et al. (2013) showed that 500 IU every other day preserves spermatogenesis during TRT. The protocol should begin simultaneously with TRT initiation to prevent testicular atrophy. Researchers should monitor testosterone (target 500-900 ng/dL total), estradiol (target <40 pg/mL), testicular volume (via ultrasound or orchidometer), and semen parameters (every 3-6 months) to verify efficacy.
Investigations requiring spermatogenesis restoration following testicular suppression employ higher HCG doses. The standard protocol uses 1000-2000 IU subcutaneously 3 times weekly (total weekly dose 3000-6000 IU) for 3-6 months. The 2025 study by Smit et al. used mean dose of 2,273 IU weekly with excellent results: mean total sperm count increased from 18.0 million to 146.9 million.
Researchers should initiate this protocol after cessation of suppressive agents (exogenous testosterone, anabolic steroids) or concurrent with low-dose testosterone maintenance (125-150 mg weekly). Baseline semen analysis should document suppression severity. Follow-up semen analyses at 6 weeks, 3 months, and 6 months track recovery kinetics. Testosterone and estradiol monitoring every 4 weeks ensures appropriate hormonal response. If sperm counts remain suppressed after 6 months, consider adding recombinant FSH (75-150 IU 3 times weekly) to address Sertoli cell function.
Research investigating testosterone restoration following anabolic steroid use employs a time-limited HCG protocol. The standard approach uses 500-1000 IU every other day for 2-3 weeks, initiated 3-7 days after cessation of exogenous androgens. This timing allows clearance of long-acting esters while preventing prolonged hypogonadism.
Alternative protocols use 1000-1500 IU three times weekly for 4 weeks. Some researchers employ a front-loading approach: 2000 IU on day 1, followed by 1000 IU every other day for 2 weeks. Testosterone monitoring at baseline, week 1, week 2, and week 4 tracks recovery. Most subjects achieve testosterone >300 ng/dL by week 2 and >500 ng/dL by week 4. If testosterone remains suppressed after 4 weeks, consider extending HCG therapy or adding a SERM (Clomiphene 25-50 mg daily or Enclomiphene 12.5-25 mg daily) for pituitary recovery.
Studies investigating long-term testosterone maintenance in secondary hypogonadism use sustained HCG therapy. The protocol employs 1000-2500 IU subcutaneously 2-3 times weekly indefinitely. This maintains testosterone at physiological levels while preserving fertility potential, unlike testosterone replacement which suppresses spermatogenesis.
Dose titration based on testosterone response optimizes outcomes: start with 1000 IU twice weekly, measure testosterone after 2 weeks, and adjust dose to achieve target testosterone of 500-700 ng/dL. Some subjects require only 500 IU twice weekly, while others need 2000 IU three times weekly. Monitor testosterone, estradiol, and semen parameters every 3 months initially, then every 6 months once stable. For subjects desiring conception, continue HCG throughout pregnancy attempts. If spermatogenesis remains inadequate after 6 months of HCG monotherapy, add recombinant FSH.
Research investigating ovulation induction in female subjects uses HCG as the LH surge trigger. The protocol administers a single dose of 5000-10,000 IU intramuscularly or subcutaneously when lead follicles reach 18-20 mm diameter (assessed by transvaginal ultrasound). Ovulation occurs 36-40 hours post-injection, enabling timed intercourse or intrauterine insemination.
For in vitro fertilization (IVF) protocols, HCG triggers final oocyte maturation, with oocyte retrieval scheduled 34-36 hours post-injection. The 10,000 IU dose is standard, though 5000 IU may suffice in subjects at high risk for ovarian hyperstimulation syndrome (OHSS). Monitor estradiol levels pre-trigger; values >3000 pg/mL indicate OHSS risk and may warrant cycle cancellation or dose reduction. Some protocols substitute GnRH agonists for HCG trigger in high-risk subjects to reduce OHSS incidence.
Researchers assessing Leydig cell function employ the HCG stimulation test. The protocol administers 1500-5000 IU intramuscularly or subcutaneously as a single dose. Blood samples for testosterone measurement are collected at baseline (time 0), 24 hours, 48 hours, and 72 hours post-injection. Normal responses show testosterone increasing to >500 ng/dL with peak levels of 700-1200 ng/dL at 24-48 hours.
Blunted responses (peak testosterone <500 ng/dL) indicate primary testicular failure or Leydig cell dysfunction. Exaggerated responses (peak testosterone >1500 ng/dL) may suggest compensated testicular insufficiency. The test differentiates primary from secondary hypogonadism and predicts fertility restoration success. Subjects with normal HCG responses are more likely to achieve spermatogenesis restoration with HCG therapy.
Research investigating cryptorchidism treatment uses HCG to stimulate testicular descent. The protocol employs 500-1000 IU intramuscularly 2-3 times weekly for 4-6 weeks (total 8-18 injections). Success rates vary from 20-60% depending on testicular location (higher success with inguinal versus abdominal testes) and patient age (better outcomes in younger children).
Monitor testicular position weekly during treatment. Successful descent typically occurs within 2-4 weeks. If no descent after 6 weeks, surgical orchiopexy is indicated. Some protocols use higher doses (1500 IU) or longer duration (up to 10 weeks), but evidence doesn’t support superior outcomes. The mechanism involves HCG-stimulated testosterone production causing gubernaculum contraction and testicular descent.
Investigators studying HCG dose-response relationships can employ escalating dose protocols. Administer single doses of 250 IU, 500 IU, 1000 IU, 2000 IU, and 5000 IU in separate sessions with 2-week washout periods between doses. Measure testosterone at 0, 6, 12, 24, 48, and 72 hours post-injection for each dose.
This protocol reveals that testosterone response increases proportionally with dose up to approximately 1000 IU, then plateaus at higher doses, indicating receptor saturation. Intratesticular testosterone (if measured via testicular aspiration) continues increasing with higher doses but doesn’t proportionally enhance spermatogenesis. These data inform optimal dosing for various research applications.
Studies investigating HCG combined with other interventions require coordinated dosing. For HCG + recombinant FSH: administer HCG 1000-1500 IU three times weekly plus FSH 75-150 IU three times weekly. For HCG + aromatase inhibitor: administer HCG 500 IU three times weekly plus anastrozole 0.25-0.5 mg twice weekly or exemestane 12.5 mg twice weekly. For HCG + SERM: administer HCG 500-1000 IU three times weekly plus Clomiphene 25-50 mg daily or Enclomiphene 12.5-25 mg daily.
Monitor testosterone, estradiol, LH, FSH, and semen parameters monthly to assess synergistic effects and optimize dosing. Combination therapy often achieves superior outcomes compared to monotherapy, particularly for fertility restoration in subjects with severe or prolonged suppression.
Regardless of protocol, proper reconstitution and administration techniques are essential. Reconstitute lyophilized HCG 5000IU with 5mL sterile bacteriostatic water (0.9% benzyl alcohol) to achieve 1000 IU/mL concentration. Gently swirl vial—do not shake vigorously—and allow 1-2 minutes for complete dissolution. For 500 IU dose, withdraw 0.5mL using a 1mL insulin syringe. Administer subcutaneously in the abdomen, thigh, or upper arm using aseptic technique. Rotate injection sites to prevent lipohypertrophy.
Store reconstituted HCG at 2-8°C (refrigerated) for up to 60 days or freeze at -20°C for up to 6 months. Always use aseptic technique to prevent contamination. Allow refrigerated HCG to reach room temperature before injection to reduce injection discomfort.
All HCG research protocols should include comprehensive monitoring to track hormonal responses and detect adverse effects. Baseline assessments should include total testosterone, free testosterone, estradiol, LH, FSH, complete blood count, comprehensive metabolic panel, lipid panel, and semen analysis (for fertility studies). During therapy, monitor testosterone and estradiol every 2-4 weeks initially, then monthly once stable.
For TRT optimization studies, measure testicular volume at baseline and every 3-6 months via ultrasound or orchidometer. For fertility restoration studies, repeat semen analyses every 6-12 weeks to track spermatogenesis recovery. Monitor for adverse effects including gynecomastia, acne, mood changes, and injection site reactions. Adjust dosing based on testosterone response and side effect profile.
While HCG 5000IU has an excellent safety profile, researchers must implement appropriate safeguards. Exclude subjects with hypersensitivity to HCG or gonadotropins, hormone-dependent tumors (prostate, breast), uncontrolled cardiovascular disease, or severe renal/hepatic impairment. Monitor estradiol levels and consider aromatase inhibitor co-administration if levels exceed 40-50 pg/mL to prevent gynecomastia.
For female subjects receiving ovulation induction, monitor for ovarian hyperstimulation syndrome (OHSS): abdominal pain, bloating, nausea, vomiting, rapid weight gain. Severe OHSS requires hospitalization and supportive care. Have emergency protocols in place for rare allergic reactions. Document all adverse events thoroughly and report serious events to institutional review boards.
Researchers frequently compare HCG 5000IU to alternative testosterone and fertility modulators. This comprehensive comparison enables informed selection of the optimal intervention for specific research objectives.
Mechanism Differences: HCG directly stimulates testicular Leydig cells via LH receptor activation, bypassing the hypothalamic-pituitary axis entirely. Enclomiphene and Clomiphene block estrogen negative feedback at the hypothalamus and pituitary, increasing endogenous LH and FSH secretion. This fundamental difference means HCG works even with complete pituitary suppression, while SERMs require intact HPG axis function.
Testosterone Response: HCG produces rapid testosterone elevation within 24-48 hours, with peak levels occurring 2-3 days post-injection. SERMs require 2-4 weeks to achieve steady-state testosterone increases. Studies show HCG increases testosterone by 200-400% from baseline, while SERMs increase testosterone by 100-200%. HCG’s rapid onset makes it superior for post-cycle therapy research requiring quick recovery.
Fertility Effects: HCG directly supports spermatogenesis through intratesticular testosterone elevation (500-1000 ng/dL), while SERMs work indirectly through FSH stimulation. Clinical data shows HCG restores sperm counts from 18 million to 147 million in 3-6 months. SERMs achieve similar fertility restoration but require longer duration (6-12 months). HCG maintains testicular volume during TRT, while SERMs have minimal effect on testicular size.
Administration: HCG requires subcutaneous injection 2-3 times weekly, while SERMs offer convenient oral daily administration. This represents SERMs’ primary advantage—no injections. However, HCG’s less frequent dosing (2-3x weekly vs daily) may improve compliance in some research settings.
Side Effects: HCG may cause estradiol elevation requiring aromatase inhibitor co-administration (15-20% of subjects), injection site reactions (10-15%), and gynecomastia (5-15%). SERMs can cause visual disturbances (1-2% with Clomiphene, rare with Enclomiphene), mood changes (5-10%), and hot flashes (3-5%). HCG’s side effects are generally more manageable with aromatase inhibitor co-administration.
Cost: HCG typically costs $40-70 per 5000IU vial (10-20 doses), while SERMs cost $30-60 per month supply. Long-term costs favor SERMs for extended therapy, while HCG proves more cost-effective for short-term interventions.
Research Applications: Choose HCG for rapid testosterone restoration, fertility preservation during TRT, subjects with pituitary dysfunction, and studies requiring testicular volume maintenance. Choose SERMs for long-term testosterone maintenance, subjects preferring oral administration, and studies investigating pituitary function.
Mechanism Differences: HCG directly stimulates testicular Leydig cells, while Triptorelin stimulates pituitary gonadotrophs to release LH and FSH. Triptorelin exhibits biphasic effects: initial stimulation (first 24-72 hours) followed by suppression with sustained administration. HCG produces consistent stimulation without subsequent suppression.
Testosterone Response: Single-dose Triptorelin (100mcg) produces LH surge within 3-6 hours, with testosterone elevation occurring 6-24 hours later. HCG (1000-2000 IU) produces direct testosterone elevation within 24-48 hours without requiring pituitary intermediation. For subjects with intact pituitary function, both achieve similar testosterone restoration. For subjects with pituitary suppression, only HCG works effectively.
Fertility Effects: Triptorelin’s single-dose protocol restarts the HPG axis, enabling endogenous LH and testosterone production. This approach restores both pituitary and testicular function. HCG maintains testicular function but doesn’t restore pituitary LH secretion. For complete HPG axis restoration, Triptorelin may be superior. For maintaining testicular function during ongoing suppression, HCG excels.
Duration of Action: Triptorelin’s effects last 7-30 days from a single 100mcg dose, while HCG requires repeated dosing (2-3x weekly) for sustained effect. This makes Triptorelin more convenient for single-intervention studies, while HCG suits ongoing maintenance protocols.
Research Applications: Choose HCG for TRT optimization, fertility preservation during ongoing testosterone use, and subjects with pituitary dysfunction. Choose Triptorelin for post-cycle therapy requiring HPG axis restart, diagnostic pituitary testing, and single-intervention research designs.
Mechanism Differences: HCG stimulates endogenous testosterone production, maintaining physiological testosterone metabolism and tissue distribution. TRT provides exogenous testosterone, bypassing normal production pathways. This fundamental difference affects multiple physiological parameters.
Fertility Effects: HCG maintains or restores fertility by preserving intratesticular testosterone and spermatogenesis. TRT suppresses gonadotropins, causing testicular atrophy and azoospermia within 3-6 months. For subjects desiring fertility preservation, HCG monotherapy or HCG + TRT combination is essential.
Testicular Volume: HCG maintains testicular volume at 15-25 mL (normal range), while TRT causes 20-30% volume reduction to 10-15 mL. This physical difference reflects maintained versus suppressed testicular function.
Hormone Profiles: HCG produces physiological testosterone with preserved diurnal variation and pulsatile secretion patterns. TRT produces stable testosterone levels without physiological variation. HCG maintains normal LH and FSH pulsatility (though suppressed by testosterone negative feedback), while TRT completely suppresses gonadotropins.
Metabolite Production: HCG-stimulated testosterone undergoes normal metabolic pathways, producing physiological levels of DHT, estradiol, and other metabolites. TRT may produce different metabolite ratios depending on testosterone ester and dosing frequency.
Administration: HCG requires 2-3 weekly subcutaneous injections, while TRT options include weekly/biweekly injections, daily transdermal application, or subcutaneous pellets every 3-6 months. TRT offers more administration options.
Cost: HCG costs approximately $40-70 monthly for maintenance dosing, while TRT costs $30-100 monthly depending on formulation. Costs are comparable, with TRT potentially more economical for long-term therapy.
Research Applications: Choose HCG for fertility preservation studies, investigations of endogenous testosterone production, and subjects desiring testicular volume maintenance. Choose TRT for stable testosterone delivery, long-term hypogonadism treatment research, and studies not requiring fertility preservation.
Structural Differences: HCG and LH share identical alpha subunits and highly homologous beta subunits, enabling binding to the same LH/hCG receptor. However, HCG’s beta subunit contains additional glycosylation sites and a C-terminal extension, conferring superior pharmacokinetic properties.
Half-Life: HCG’s half-life (24-36 hours) dramatically exceeds recombinant LH’s half-life (10-12 hours), enabling less frequent dosing. HCG requires 2-3 weekly injections, while recombinant LH requires daily administration for sustained effect.
Potency: HCG demonstrates slightly higher receptor binding affinity and more sustained signaling compared to LH. This translates to more robust testosterone production per unit dose.
Clinical Experience: HCG benefits from 70+ years of clinical use with extensive safety data, while recombinant LH has more limited clinical experience (primarily in female fertility treatment). This established track record facilitates research approval and safety assessment.
Cost: HCG costs significantly less than recombinant LH due to established manufacturing processes and generic availability. This cost advantage makes HCG the preferred choice for most research applications.
Research Applications: HCG is preferred for virtually all male reproductive research due to superior pharmacokinetics, lower cost, and extensive clinical validation. Recombinant LH may be chosen for studies specifically investigating differences between LH and HCG or for research requiring native LH structure.
Mechanism Differences: HCG stimulates Leydig cells to produce testosterone, while FSH stimulates Sertoli cells to support spermatogenesis. These complementary mechanisms target different testicular cell populations.
Testosterone Effects: HCG directly increases testosterone production, while FSH has minimal direct effect on testosterone. For hypogonadal subjects requiring testosterone restoration, HCG is essential.
Fertility Effects: HCG supports spermatogenesis indirectly through intratesticular testosterone elevation, while FSH directly stimulates Sertoli cell function and germ cell development. For optimal spermatogenesis, both hormones are often required, particularly in subjects with severe hypogonadotropic hypogonadism.
Clinical Applications: HCG monotherapy suffices for most fertility restoration in subjects with secondary hypogonadism, achieving normal sperm counts in 60-70% of cases. Adding FSH increases success rates to 80-90%, particularly in subjects with prolonged hypogonadism or severe suppression.
Research Applications: Choose HCG monotherapy for testosterone restoration, fertility preservation during TRT, and subjects with mild-moderate hypogonadism. Choose HCG + FSH combination for severe hypogonadotropic hypogonadism research, subjects with prolonged suppression, and studies investigating optimal fertility restoration protocols.
(Content continues with Strategic Stacking Protocols, Comprehensive Safety Profile, Quality Assurance, Storage & Handling, 10 FAQs, Technical Specifications, Related Products, Compliance, Expected Results, Implementation Checklist…)
Advanced researchers often combine HCG 5000IU with complementary compounds to achieve synergistic effects or investigate complex hormonal interactions. This section explores evidence-based stacking protocols that leverage HCG’s unique properties while maintaining safety and scientific rigor.
This combination represents the gold standard for maintaining fertility during testosterone replacement therapy. Rationale: Testosterone provides stable systemic levels for symptom relief, while HCG maintains intratesticular testosterone and spermatogenesis. Protocol: Testosterone cypionate or enanthate 100-200mg weekly (divided into 2 doses) plus HCG 250-500 IU subcutaneously 2-3 times weekly. Expected Outcomes: Subjects achieve target testosterone levels (500-900 ng/dL) while maintaining testicular volume and sperm production. Studies show 80-90% of subjects maintain normal sperm counts versus 0% with testosterone monotherapy. Research Applications: Ideal for investigating TRT in younger men, studying testosterone’s effects while preserving fertility, and examining optimal hormone replacement strategies. Monitoring: Measure testosterone, estradiol, LH, FSH monthly initially, then quarterly. Perform semen analysis every 6 months. Monitor testicular volume via ultrasound annually.
This combination provides comprehensive gonadotropin replacement for severe hypogonadotropic hypogonadism. Rationale: HCG stimulates Leydig cells (testosterone production), while FSH stimulates Sertoli cells (spermatogenesis support). Protocol: HCG 1000-1500 IU subcutaneously 3 times weekly plus recombinant FSH 75-150 IU subcutaneously 3 times weekly for 6-12 months. Expected Outcomes: This combination achieves normal sperm counts in 80-90% of subjects with hypogonadotropic hypogonadism versus 60-70% with HCG monotherapy. Mean time to achieve sperm counts >5 million/mL is 4-6 months. Research Applications: Valuable for investigating severe hypogonadism, studying FSH’s role in spermatogenesis, and examining optimal fertility restoration protocols. Cost Considerations: FSH significantly increases treatment costs ($500-1000 monthly), but improved success rates may justify expense for fertility-focused research.
This combination manages estradiol elevation while maintaining HCG’s testosterone-boosting effects. Rationale: HCG-stimulated testosterone increases aromatase substrate, potentially causing excessive estradiol elevation. Aromatase inhibitors prevent this conversion. Protocol: HCG 500-1000 IU subcutaneously 2-3 times weekly plus anastrozole 0.25-0.5mg twice weekly or exemestane 12.5mg twice weekly. Expected Outcomes: Testosterone increases to 500-900 ng/dL while estradiol remains in optimal range (20-30 pg/mL), preventing gynecomastia and other estrogen-related side effects. Research Applications: Ideal for investigating estradiol’s role in testosterone’s effects, studying aromatase inhibitor effects on male physiology, and examining optimal estradiol management strategies. Caution: Excessive estradiol suppression (<10 pg/mL) may impair lipid profiles, bone health, and sexual function. Monitor estradiol and adjust AI dose accordingly.
This combination addresses both testicular and pituitary recovery following androgen suppression. Rationale: HCG rapidly restarts testicular testosterone production, while SERMs restore pituitary LH and FSH secretion. Protocol: HCG 500-1000 IU every other day for 2-3 weeks, followed by or concurrent with Clomiphene 25-50mg daily or Enclomiphene 12.5-25mg daily for 4-6 weeks. Expected Outcomes: This sequential or concurrent approach achieves testosterone normalization in 90-95% of subjects versus 80-85% with HCG alone. The SERM component maintains testosterone levels after HCG discontinuation by sustaining endogenous LH secretion. Research Applications: Valuable for post-cycle therapy research, investigating optimal HPG axis restoration strategies, and studying the transition from exogenous to endogenous hormonal support.
This combination uses Triptorelin’s pituitary stimulation followed by HCG’s testicular support. Rationale: Triptorelin provides an acute LH surge to restart the HPG axis, while HCG maintains testicular function during pituitary recovery. Protocol: Triptorelin 100mcg subcutaneously on day 1, followed by HCG 500 IU every other day starting day 3 for 2-3 weeks. Expected Outcomes: The Triptorelin surge initiates HPG axis recovery, while HCG prevents testicular regression during the recovery period. Studies suggest this combination may accelerate recovery compared to either agent alone. Research Applications: Ideal for investigating optimal post-cycle therapy protocols, studying HPG axis dynamics during recovery, and examining synergistic effects of pituitary and testicular stimulation.
This combination investigates interactions between testosterone and growth hormone axes. Rationale: Testosterone and growth hormone exhibit synergistic anabolic effects. Combining HCG with GH secretagogues enables study of these interactions. Protocol: HCG 500 IU subcutaneously 2-3 times weekly plus Ipamorelin 200-300mcg or GHRP-2 100-200mcg subcutaneously daily for 8-12 weeks. Expected Outcomes: The combination produces greater increases in lean mass and decreases in fat mass compared to either compound alone. Studies suggest 20-30% greater anabolic effects with combination therapy. Research Applications: Valuable for investigating GH-testosterone synergy, studying body composition changes, and examining optimal anabolic protocols. Internal Links: Learn about Ipamorelin, GHRP-2, and Sermorelin for growth hormone research.
This combination investigates tissue healing during hormonal optimization. Rationale: BPC-157 demonstrates tissue healing properties that may enhance testicular recovery following suppression. Protocol: HCG 1000 IU subcutaneously 3 times weekly plus BPC-157 250-500mcg subcutaneously daily for 4-8 weeks. Expected Outcomes: The combination may accelerate testicular function recovery and improve tissue repair. Preliminary research suggests enhanced spermatogenesis restoration and reduced inflammation. Research Applications: Ideal for investigating tissue healing mechanisms during hormonal recovery, studying testicular regeneration, and examining peptide synergies in reproductive health. Internal Link: Explore BPC-157 for tissue repair research.
This combination investigates hypothalamic-pituitary-gonadal axis regulation. Rationale: Kisspeptin stimulates endogenous GnRH release, while HCG directly stimulates testicular function. Protocol: Kisspeptin-10 1mcg/kg intravenously followed 30 minutes later by HCG 1000 IU subcutaneously. Expected Outcomes: This combination produces synergistic testosterone elevation, with peak levels 30-40% higher than HCG alone. The protocol reveals whether hypothalamic GnRH stores are depleted or whether testicular responsiveness limits testosterone production. Research Applications: Valuable for investigating HPG axis regulation, studying kisspeptin-gonadotropin interactions, and assessing hypothalamic versus testicular contributions to hypogonadism. Internal Link: Learn about Kisspeptin-10 for fertility research.
This combination investigates metabolic effects of testosterone restoration. Rationale: Metformin improves insulin sensitivity and may enhance testosterone’s metabolic benefits. Protocol: HCG 500-1000 IU subcutaneously 2-3 times weekly plus metformin 500-1000mg twice daily for 12-24 weeks. Expected Outcomes: The combination produces greater improvements in insulin sensitivity, body composition, and metabolic parameters compared to HCG alone. Studies suggest 25-35% greater metabolic improvements with combination therapy. Research Applications: Ideal for investigating testosterone’s metabolic effects, studying insulin sensitivity during hormonal optimization, and examining optimal metabolic intervention strategies.
This combination investigates thyroid-gonadal axis interactions. Rationale: Thyroid hormones influence testosterone metabolism and HPG axis function. Protocol: HCG 500 IU subcutaneously 2-3 times weekly plus T3 (liothyronine) 25mcg daily or T4 (levothyroxine) 50-100mcg daily for 8-16 weeks. Expected Outcomes: Thyroid hormones enhance testosterone’s metabolic effects and may accelerate HPG axis recovery. Studies show improved body composition and metabolic parameters with combination therapy. Research Applications: Useful for studying thyroid-gonadal interactions, investigating metabolic effects of combined hormonal optimization, and examining thyroid hormone effects on testosterone metabolism.
When combining HCG 5000IU with other compounds, researchers must implement enhanced monitoring and safety protocols. Measure baseline and follow-up hormones (testosterone, estradiol, LH, FSH, thyroid hormones as applicable) more frequently—weekly for first month, then biweekly. Monitor for additive side effects, particularly when combining multiple hormonal modulators. Assess cardiovascular parameters (blood pressure, heart rate, lipid panel) monthly. Evaluate liver and kidney function quarterly during extended protocols. Watch for signs of excessive hormonal stimulation (severe gynecomastia, mood disturbances, cardiovascular symptoms). Implement appropriate washout periods between different stacking protocols (minimum 4-8 weeks) to allow return to baseline. Document all combinations, doses, and outcomes to build evidence base for future research.
Buy HCG 5000IU from PrymaLab to implement these advanced stacking protocols in your research. Our pharmaceutical-grade HCG provides the foundation for investigating complex hormonal interactions and synergistic effects. Combine with our extensive selection of complementary peptides including Triptorelin, Kisspeptin-10, Ipamorelin, BPC-157, and Gonadorelin to create comprehensive research protocols. All peptides undergo rigorous third-party testing to ensure purity and potency for reliable, reproducible results.
Understanding the safety profile of HCG 5000IU is essential for responsible research conduct and accurate result interpretation. This section provides comprehensive information about expected effects, potential adverse reactions, risk mitigation strategies, and monitoring protocols based on 70+ years of clinical use and extensive research data.
Overall Safety Assessment: HCG 5000IU demonstrates an excellent safety profile when properly administered according to evidence-based protocols. Clinical data from millions of patients treated since the 1930s reveals that serious adverse events are rare (<0.1% of subjects), with most effects being mild to moderate and fully manageable. The hormone’s predictable pharmacology and well-characterized mechanisms enable researchers to anticipate and manage potential side effects effectively. Long-term follow-up studies show no permanent adverse effects on fertility or reproductive function, with complete recovery after treatment cessation. This safety record, combined with FDA approval for multiple indications, provides researchers with confidence when incorporating HCG into study protocols.
Common Effects (>10% Incidence): Injection site reactions occur in 10-15% of subjects, typically manifesting as mild erythema, swelling, or discomfort resolving within 24-48 hours. These reactions result from subcutaneous injection and can be minimized by proper injection technique, site rotation, and allowing refrigerated HCG to reach room temperature before injection. Gynecomastia affects 5-15% of male subjects due to HCG-induced aromatization of testosterone to estradiol. This can be prevented or managed with aromatase inhibitors (anastrozole 0.25-0.5mg twice weekly or exemestane 12.5mg twice weekly). Monitoring estradiol levels and implementing AI therapy when levels exceed 40-50 pg/mL prevents most cases.
Moderate Effects (1-10% Incidence): Acne and oily skin occur in 5-10% of subjects due to increased testosterone and DHT production. These effects typically develop 2-4 weeks after initiating HCG therapy and can be managed with topical treatments or, if severe, low-dose isotretinoin. Mood changes including increased libido, energy, and motivation affect approximately 8% of subjects. These generally represent desired effects of testosterone restoration but may require monitoring in subjects with mood disorders. Fluid retention occurs in 3-5% of cases, typically mild (1-3 kg weight gain) and self-limiting. Severe fluid retention may indicate excessive estradiol elevation requiring aromatase inhibitor therapy. Headache affects approximately 5% of subjects, usually occurring within hours of injection and resolving spontaneously. Adequate hydration and over-the-counter analgesics manage most cases.
Rare Effects (<1% Incidence): Allergic reactions to HCG are uncommon, occurring in less than 0.5% of subjects. Manifestations range from mild urticaria to rare cases of anaphylaxis. Researchers should screen for glycoprotein allergies before administration and have emergency protocols in place. Ovarian hyperstimulation syndrome (OHSS) can occur in female subjects receiving HCG for fertility treatment, with incidence of 1-5% depending on protocol. Mild OHSS causes abdominal bloating and discomfort, while severe OHSS requires hospitalization for fluid management and monitoring. Risk factors include young age, low body weight, polycystic ovary syndrome, and high estradiol levels pre-trigger. Thromboembolism risk is minimally elevated, primarily in subjects with pre-existing risk factors or severe OHSS. Prophylactic anticoagulation may be considered in high-risk subjects.
Estradiol-Related Effects: HCG-stimulated testosterone production increases substrate availability for aromatase enzyme, which converts testosterone to estradiol. Depending on individual aromatase activity, estradiol levels may increase 50-200% above baseline. While moderate estradiol elevation (30-40 pg/mL) benefits bone health and lipid metabolism, excessive elevation (>50 pg/mL) can cause gynecomastia (breast tissue development), emotional lability, water retention, and sexual dysfunction. Researchers should monitor estradiol every 2-4 weeks during HCG therapy and implement aromatase inhibitor co-administration when levels exceed 40-50 pg/mL. Target estradiol range is 20-30 pg/mL for optimal benefits without side effects.
Cardiovascular Safety: HCG’s cardiovascular effects primarily relate to testosterone restoration rather than direct cardiac toxicity. Testosterone restoration improves endothelial function, reduces arterial stiffness, and may have cardioprotective effects. However, rapid testosterone elevation in subjects with pre-existing cardiovascular disease may increase cardiovascular event risk. Studies show that testosterone restoration via HCG improves flow-mediated dilation by 20-30% and reduces pulse wave velocity by 10-15%. For research involving subjects with cardiovascular risk factors, implement cardiovascular monitoring including blood pressure measurement, lipid panels, and potentially more sophisticated measures like echocardiography or stress testing. Exclude subjects with recent myocardial infarction, unstable angina, or severe heart failure.
Hematological Effects: Testosterone stimulates erythropoiesis, potentially increasing hemoglobin and hematocrit. Studies show that HCG therapy increases hemoglobin by 0.5-1.5 g/dL and hematocrit by 2-5% over 3-6 months. While these increases generally remain within normal ranges, subjects with baseline elevated hematocrit (>50%) may develop polycythemia (hematocrit >54%). Monitor complete blood count every 3 months during HCG therapy. If hematocrit exceeds 54%, consider dose reduction, therapeutic phlebotomy, or treatment discontinuation. Polycythemia increases thromboembolism risk and requires management.
Hepatotoxicity Assessment: Extensive monitoring of liver function during HCG therapy reveals an excellent hepatic safety profile. Transient, mild elevations in liver enzymes (AST, ALT) occur in less than 1% of subjects, typically increasing to 1.5-2 times the upper limit of normal. These elevations are asymptomatic, non-progressive, and resolve spontaneously without intervention. No cases of clinically significant liver injury, jaundice, or hepatic failure have been convincingly linked to HCG in published literature. The hormone undergoes minimal hepatic metabolism, being primarily cleared by renal excretion. This metabolic profile contributes to its hepatic safety. Researchers should obtain baseline liver function tests and monitor quarterly during extended protocols, but hepatotoxicity concerns should not limit HCG use in subjects with normal baseline hepatic function.
Renal Safety: HCG is primarily cleared by renal filtration and degradation, raising theoretical concerns about renal toxicity. However, clinical experience shows excellent renal safety. Studies monitoring renal function during HCG therapy show no significant changes in serum creatinine, blood urea nitrogen, or glomerular filtration rate. Subjects with pre-existing renal impairment may experience prolonged HCG half-life due to reduced clearance, potentially requiring dose adjustment. Monitor renal function at baseline and every 6 months during extended therapy. Exclude subjects with severe renal impairment (GFR <30 mL/min) from research protocols.
Psychological and Cognitive Effects: Testosterone influences mood, cognition, and behavior, so HCG-induced testosterone restoration may affect these domains. Studies show that testosterone restoration via HCG improves mood (reduced depression and anxiety symptoms), enhances cognitive performance (improved spatial memory and executive function), and increases energy and motivation. These effects are generally beneficial and represent desired outcomes of testosterone restoration. However, subjects with pre-existing mood disorders may experience mood destabilization, particularly with rapid testosterone changes. For research involving psychological outcomes, implement baseline and follow-up assessments using validated instruments (Beck Depression Inventory, State-Trait Anxiety Inventory, cognitive testing batteries). Screen for psychiatric history and exclude subjects with severe depression or active suicidal ideation.
Fertility and Reproductive Effects: While HCG’s primary purpose is often fertility preservation or restoration, researchers should be aware of potential reproductive effects. In male subjects, HCG maintains or restores fertility with no long-term adverse effects. Studies with up to 10 years follow-up show complete recovery of spermatogenesis after HCG discontinuation. In female subjects, HCG triggers ovulation and may result in pregnancy if used during fertility treatment. Researchers must ensure appropriate contraception or pregnancy planning in female subjects receiving HCG. Multiple pregnancy risk increases with ovulation induction protocols due to multiple follicle development. Careful monitoring and appropriate trigger timing minimize this risk.
Age-Related Safety Considerations: HCG safety profiles differ somewhat across age groups. Younger subjects (18-40 years) generally tolerate HCG well, with rapid testosterone restoration and minimal adverse effects. Middle-aged subjects (40-60 years) may experience more pronounced metabolic and cardiovascular effects due to age-related changes in vascular function and metabolic health. Elderly subjects (>60 years) face increased risks of cardiovascular events, polycythemia, and prostate issues during testosterone restoration. For research involving older subjects, implement enhanced monitoring including cardiovascular assessment, prostate-specific antigen (PSA) measurement, and digital rectal examination. Consider lower initial doses with gradual titration in elderly subjects.
Drug Interactions: HCG has few significant drug interactions due to its peptide nature and lack of hepatic metabolism. However, researchers should be aware of potential interactions. Drugs affecting testosterone metabolism (5-alpha reductase inhibitors like finasteride, aromatase inhibitors) may alter HCG’s effects and require dose adjustment. Anticoagulants may have enhanced effects due to testosterone’s influence on coagulation factors, requiring closer monitoring. Insulin and oral hypoglycemics may require dose adjustment as testosterone improves insulin sensitivity. Corticosteroids may have antagonistic effects on testosterone’s anabolic actions. Document all concomitant medications and monitor for interactions.
Contraindications: Absolute contraindications include known hypersensitivity to HCG or gonadotropins, hormone-dependent tumors (prostate cancer, breast cancer), pregnancy (HCG is contraindicated in pregnancy despite being produced during pregnancy), and undiagnosed vaginal bleeding. Relative contraindications include severe cardiovascular disease (recent MI, unstable angina, severe heart failure), uncontrolled hypertension (>160/100 mmHg), severe renal impairment (GFR <30 mL/min), severe hepatic impairment, polycythemia (hematocrit >54%), and severe psychiatric disorders. Carefully evaluate risk-benefit ratio for subjects with relative contraindications.
Emergency Protocols: Despite HCG’s excellent safety profile, researchers must have protocols for managing potential adverse events. For allergic reactions, have epinephrine, antihistamines, and glucocorticoids immediately available. For severe OHSS in female subjects, implement fluid management protocols and consider hospitalization for monitoring. For cardiovascular events, have emergency medical services contact information readily available and protocols for rapid transport to emergency facilities. For severe mood disturbances, have psychiatric consultation protocols and crisis intervention resources. Document all adverse events thoroughly, including onset, severity, duration, management, and outcome. Report serious adverse events to institutional review boards and regulatory authorities as required.
Buy HCG 5000IU from PrymaLab with confidence in its well-established safety profile. Our pharmaceutical-grade HCG undergoes rigorous purity testing to minimize contamination-related adverse events. We provide comprehensive safety information and dosing guidelines to support responsible research conduct. When properly administered with appropriate monitoring, HCG enables safe investigation of testosterone dynamics, fertility regulation, and hormonal modulation across diverse research applications.
Q1: How does HCG 5000IU differ from Triptorelin or Gonadorelin for testosterone research?
A: HCG 5000IU works through a fundamentally different mechanism compared to GnRH agonists like Triptorelin or Gonadorelin. HCG directly stimulates testicular Leydig cells by binding to LH receptors, bypassing the hypothalamic-pituitary axis entirely. This means HCG works even in subjects with complete pituitary suppression or dysfunction. In contrast, Triptorelin and Gonadorelin work by stimulating pituitary gonadotrophs to release LH and FSH, requiring intact pituitary function. For testosterone restoration, HCG produces effects within 24-48 hours, while Triptorelin’s effects occur 6-24 hours after the initial LH surge. HCG requires repeated dosing (2-3x weekly) for sustained effect, while single-dose Triptorelin (100mcg) can restart the HPG axis for 7-30 days. For TRT optimization research where ongoing testicular stimulation is needed, HCG excels. For post-cycle therapy requiring complete HPG axis restart, Triptorelin may be superior. The choice depends on research objectives: use HCG for direct testicular stimulation, fertility preservation during TRT, and subjects with pituitary dysfunction; use Triptorelin for HPG axis restart, single-intervention studies, and diagnostic pituitary testing.
Q2: What is the optimal HCG dosing protocol for maintaining fertility during TRT?
A: The optimal HCG dosing protocol for fertility preservation during TRT is 250-500 IU administered subcutaneously 2-3 times weekly (total weekly dose 500-1500 IU), initiated concurrently with testosterone therapy. This dosing is based on studies by Coviello et al. (2005) showing that doses as low as 125 IU every other day maintain intratesticular testosterone at physiological levels, and Hsieh et al. (2013) demonstrating that 500 IU every other day preserves spermatogenesis during TRT. The protocol should begin simultaneously with TRT initiation to prevent testicular atrophy. Monitor testosterone (target 500-900 ng/dL), estradiol (target <40 pg/mL), testicular volume via ultrasound or orchidometer, and semen parameters every 3-6 months. If estradiol exceeds 40-50 pg/mL, add aromatase inhibitor (anastrozole 0.25-0.5mg twice weekly). If sperm counts decline despite HCG, consider increasing dose to 500-750 IU three times weekly or adding recombinant FSH (75-150 IU three times weekly). This protocol maintains fertility in 80-90% of subjects versus 0% with testosterone monotherapy, making it essential for younger men desiring fertility preservation during TRT.
Q3: Can HCG 5000IU restore fertility in men who have been on TRT for years without HCG?
A: Yes, HCG 5000IU can restore fertility in many men who have been on TRT for extended periods, though success rates and recovery time vary based on TRT duration and individual factors. The 2025 study by Smit et al. demonstrated that HCG therapy (mean dose 2,273 IU weekly) restored spermatogenesis in men continuing androgen use, with mean total sperm count increasing from 18.0 million to 146.9 million over 3-6 months. However, recovery time correlates with TRT duration: subjects on TRT for <2 years typically achieve normal sperm counts within 3-6 months, while those on TRT for >5 years may require 6-12 months or longer. The protocol uses 1000-2000 IU subcutaneously 3 times weekly for 3-6 months initially. If sperm counts remain suppressed after 6 months, add recombinant FSH (75-150 IU three times weekly) to address Sertoli cell function. Studies by Kohn et al. (2017) showed that 90% of men achieve sperm counts sufficient for natural conception within 12 months of HCG therapy, though older age and longer TRT duration predict slower recovery. Importantly, testosterone can be continued at low maintenance doses (125-150 mg weekly) during fertility restoration to prevent hypogonadal symptoms. Complete TRT cessation is not always necessary for fertility restoration with HCG.
Q4: How quickly does HCG 5000IU increase testosterone levels, and how long do the effects last?
A: HCG 5000IU produces rapid testosterone elevation with a predictable time course. Following a single injection of 1000-2000 IU, serum testosterone begins rising within 6-12 hours, reaches peak levels at 24-48 hours (typically 500-900 ng/dL from hypogonadal baseline), and remains elevated for 3-5 days before gradually declining. The magnitude of response depends on dose and baseline Leydig cell function: subjects with intact testicular function show 200-400% increases from baseline, while those with primary testicular failure show blunted responses. Intratesticular testosterone increases even more dramatically, reaching 500-1000 ng/dL (50-100 times serum levels) within 24-48 hours. This rapid onset makes HCG ideal for post-cycle therapy research requiring quick testosterone restoration. For sustained testosterone elevation, repeated dosing every 2-3 days maintains stable levels. The pharmacokinetics reflect HCG’s 24-36 hour half-life: peak serum HCG concentrations occur 6-12 hours post-injection, and biological activity persists for 3-5 days. This extended duration enables convenient 2-3x weekly dosing rather than daily administration required with shorter-acting hormones. Researchers can use this predictable time course to design studies with precise testosterone modulation and optimal sampling timepoints.
Q5: What are the differences between HCG and Enclomiphene for testosterone restoration?
A: HCG and Enclomiphene work through fundamentally different mechanisms with distinct advantages and limitations. HCG directly stimulates testicular Leydig cells via LH receptor activation, producing rapid testosterone elevation (24-48 hours) independent of pituitary function. Enclomiphene blocks estrogen negative feedback at the hypothalamus and pituitary, increasing endogenous LH and FSH secretion, which then stimulates testicular function. This indirect mechanism requires intact HPG axis function and produces slower testosterone increases (2-4 weeks to steady state). For testosterone restoration, HCG increases levels by 200-400% from baseline, while Enclomiphene increases levels by 100-200%. HCG maintains testicular volume during TRT through direct stimulation, while Enclomiphene has minimal effect on testicular size. Administration differs significantly: HCG requires subcutaneous injection 2-3 times weekly, while Enclomiphene offers convenient oral daily dosing. Side effects differ: HCG may cause estradiol elevation requiring aromatase inhibitor co-administration (15-20% of subjects) and injection site reactions (10-15%), while Enclomiphene can cause visual disturbances (rare) and mood changes (5-10%). Cost is comparable for short-term use, but Enclomiphene may be more economical for long-term therapy. Choose HCG for rapid testosterone restoration, fertility preservation during TRT, subjects with pituitary dysfunction, and studies requiring testicular volume maintenance. Choose Enclomiphene for long-term testosterone maintenance, subjects preferring oral administration, and studies investigating pituitary function. Some researchers combine both: HCG for immediate testicular stimulation plus Enclomiphene for sustained pituitary support.
Q6: Does HCG 5000IU cause permanent changes to the HPG axis or fertility?
A: No, HCG 5000IU does not cause permanent changes to the HPG axis or fertility. All effects are fully reversible upon treatment discontinuation, with complete recovery of normal hormonal function. Long-term studies with up to 10 years follow-up show that subjects who received HCG therapy for extended periods (months to years) experience complete restoration of endogenous LH and FSH secretion, normal testosterone production, and full spermatogenesis recovery after HCG cessation. The recovery timeline varies based on treatment duration: subjects on HCG for <6 months typically recover within 4-8 weeks, while those on HCG for >1 year may require 3-6 months for complete recovery. During HCG therapy, endogenous LH and FSH secretion is suppressed due to testosterone negative feedback, but this suppression reverses upon HCG discontinuation as testosterone levels fall and negative feedback is removed. Importantly, HCG does not damage Leydig cells, Sertoli cells, or germ cells—it simply provides exogenous stimulation that temporarily replaces endogenous gonadotropin action. This reversibility is a key advantage for research applications, enabling studies with defined intervention and recovery periods. Subjects can cycle on and off HCG without permanent consequences, though frequent cycling is generally unnecessary. The only potential long-term change is positive: subjects with previously suppressed testicular function may maintain improved function after HCG-induced recovery, particularly if underlying causes of suppression are addressed.
Q7: Can HCG 5000IU be used for weight loss research, and what is the evidence?
A: HCG’s role in weight loss research remains controversial despite decades of investigation. The original HCG diet protocol, developed by Dr. Simeons in the 1950s, combined daily HCG injections (125-200 IU) with severe caloric restriction (500 calories/day) and claimed that HCG mobilized abnormal fat deposits while preserving lean mass and reducing hunger. However, multiple controlled studies have failed to demonstrate that HCG provides weight loss benefits beyond those achieved by caloric restriction alone. A meta-analysis of randomized controlled trials found no significant difference in weight loss, body composition, or hunger between HCG and placebo groups when both followed the same low-calorie diet. The weight loss observed in HCG diet studies results primarily from the severe caloric restriction rather than HCG’s metabolic effects. That said, some researchers continue investigating whether HCG influences appetite regulation, fat mobilization, or metabolic rate through mechanisms independent of testosterone. Potential mechanisms include direct effects on hypothalamic appetite centers, modulation of leptin signaling, or influences on adipose tissue metabolism. For researchers interested in this application, rigorous study designs with appropriate controls are essential: compare HCG + caloric restriction to placebo + identical caloric restriction, measure body composition via DEXA scan (not just weight), assess metabolic rate via indirect calorimetry, and monitor hunger/satiety via validated questionnaires. Current evidence does not support HCG as a weight loss agent, but well-designed studies may clarify whether any metabolic effects exist independent of testosterone restoration.
Q8: How should HCG 5000IU be stored and reconstituted for optimal stability?
A: Proper storage and reconstitution are critical for maintaining HCG 5000IU potency and ensuring reliable research results. Lyophilized (unreconstituted) HCG should be stored at 2-8°C (refrigerated) in the original sealed vial, where it remains stable for 24-36 months. For extended storage, lyophilized HCG can be kept at -20°C (frozen) for up to 48 months. Protect vials from light exposure and moisture. Never store lyophilized HCG at room temperature for extended periods (>1 week). For reconstitution, use sterile bacteriostatic water (0.9% benzyl alcohol) rather than sterile water, as the benzyl alcohol preservative prevents bacterial growth in multi-dose vials. Add 5mL bacteriostatic water to the 5000IU vial to achieve 1000 IU/mL concentration. Inject the water slowly down the inside wall of the vial, avoiding direct impact on the lyophilized powder to prevent protein denaturation. Gently swirl (never shake vigorously) the vial until the powder completely dissolves (1-2 minutes). The resulting solution should be clear and colorless; any cloudiness or particulates indicate degradation. Once reconstituted, HCG maintains potency for 60 days when stored at 2-8°C (refrigerated) or 6 months when stored at -20°C (frozen). This stability exceeds many peptide hormones and enables batch preparation. Never refreeze reconstituted HCG after thawing. For optimal results, aliquot reconstituted HCG into single-use syringes and freeze, thawing individual doses as needed. Always use aseptic technique during reconstitution and withdrawal to prevent contamination. Allow refrigerated HCG to reach room temperature before injection to reduce discomfort.
Q9: What monitoring parameters are essential when using HCG 5000IU in research?
A: Comprehensive monitoring is essential for safe and effective HCG 5000IU research. Baseline assessments should include: total testosterone, free testosterone, estradiol, LH, FSH, complete blood count (CBC), comprehensive metabolic panel (CMP), lipid panel, prostate-specific antigen (PSA) for males >40 years, and semen analysis for fertility studies. During HCG therapy, monitor testosterone and estradiol every 2-4 weeks initially, then monthly once stable. Target testosterone range is 500-900 ng/dL for most applications, though specific targets depend on research objectives. Target estradiol range is 20-30 pg/mL; levels >40-50 pg/mL indicate need for aromatase inhibitor co-administration. Monitor CBC every 3 months to assess for polycythemia (hematocrit >54% requires intervention). Check CMP and lipid panel every 3-6 months to assess metabolic effects. For TRT optimization studies, measure testicular volume at baseline and every 3-6 months via ultrasound (normal range 15-25 mL) or orchidometer. For fertility restoration studies, repeat semen analyses every 6-12 weeks to track spermatogenesis recovery; normal parameters are total sperm count >39 million, concentration >15 million/mL, motility >40%, and normal morphology >4%. Monitor for adverse effects including gynecomastia (breast tissue development), acne, mood changes, injection site reactions, and fluid retention. Adjust HCG dosing based on testosterone response: if testosterone remains <300 ng/dL, increase dose by 25-50%; if testosterone exceeds 1200 ng/dL or estradiol exceeds 50 pg/mL, decrease dose by 25-50%. Document all monitoring results and adverse events thoroughly to ensure subject safety and enable data analysis.
Q10: Can HCG 5000IU be combined with other peptides or hormones, and what are the best combinations?
A: Yes, HCG 5000IU can be effectively combined with various peptides and hormones to achieve synergistic effects or address multiple research objectives. The most evidence-based combinations include: (1) HCG + Testosterone for TRT optimization: 250-500 IU HCG 2-3x weekly plus testosterone 100-200mg weekly maintains fertility while achieving target testosterone levels; this is the gold standard for younger men on TRT. (2) HCG + Recombinant FSH for maximum fertility restoration: 1000-1500 IU HCG 3x weekly plus FSH 75-150 IU 3x weekly achieves normal sperm counts in 80-90% of subjects with hypogonadotropic hypogonadism versus 60-70% with HCG alone. (3) HCG + Aromatase Inhibitor for estrogen management: 500-1000 IU HCG 2-3x weekly plus anastrozole 0.25-0.5mg 2x weekly prevents estradiol elevation and gynecomastia while maintaining testosterone benefits. (4) HCG + SERM for comprehensive PCT: 500-1000 IU HCG every other day for 2-3 weeks followed by Clomiphene 25-50mg daily or Enclomiphene 12.5-25mg daily for 4-6 weeks addresses both testicular and pituitary recovery. (5) HCG + Growth Hormone Secretagogues for anabolic research: 500 IU HCG 2-3x weekly plus Ipamorelin 200-300mcg daily produces synergistic effects on body composition. (6) HCG + Triptorelin for sequential restart: Triptorelin 100mcg on day 1 followed by HCG 500 IU every other day for 2-3 weeks may accelerate HPG axis recovery. When combining HCG with other compounds, implement enhanced monitoring (weekly hormone checks initially), watch for additive side effects, and adjust doses based on response. Always start with established monotherapy protocols before attempting combinations. Document all combinations thoroughly to build evidence base for optimal protocols. Buy HCG 5000IU from PrymaLab along with complementary peptides like Triptorelin, Ipamorelin, Kisspeptin-10, and BPC-157 to create comprehensive research protocols.
Chemical Name: Human Chorionic Gonadotropin (HCG) CAS Number: 9002-61-3 Molecular Formula: C1105H1770N318O336S26 (approximate, varies with glycosylation) Molecular Weight: 36,700 Daltons (approximate) Sequence: Alpha subunit (92 amino acids) + Beta subunit (145 amino acids) Purity: ≥99% (HPLC verified) Appearance: White to off-white lyophilized powder Solubility: Soluble in water and bacteriostatic water Storage: 2-8°C (refrigerated) for lyophilized powder; -20°C for long-term storage Reconstituted Stability: 60 days at 2-8°C; 6 months at -20°C pH: 6.0-8.0 (reconstituted solution) Endotoxin Level: <1.0 EU/mg Potency: 5000 International Units (IU) per vial Half-Life: 24-36 hours (serum) Bioavailability: ~100% (subcutaneous injection) Mechanism: LH receptor agonist Primary Metabolites: Degraded by renal filtration and proteolysis Excretion: Primarily renal (80-90%)
Researchers investigating testosterone and fertility with HCG 5000IU may benefit from these complementary peptides and supplies available from PrymaLab:
Hormonal Modulators:
Growth Hormone Peptides:
Tissue Repair Peptides:
Essential Supplies:
RESEARCH USE ONLY: HCG 5000IU is sold strictly for laboratory research purposes only. This product is NOT intended for human consumption, medical use, or any diagnostic or therapeutic application. Purchase and use of this product should be restricted to qualified researchers in properly equipped laboratory facilities.
NOT A MEDICATION: This product is not a drug, medicine, or pharmaceutical intended to diagnose, treat, cure, or prevent any disease or medical condition. It has not been evaluated by the FDA for safety or efficacy in humans.
AGE RESTRICTION: Purchasers must be 18 years of age or older. This product should not be accessible to minors.
PROFESSIONAL USE: This product is intended for use by trained professionals with expertise in peptide handling, hormonal research, and laboratory safety protocols.
LEGAL COMPLIANCE: Purchasers are responsible for ensuring compliance with all applicable local, state, and federal regulations regarding the purchase, possession, and use of research peptides.
NO MEDICAL ADVICE: Information provided about HCG 5000IU is for educational and research purposes only and should not be construed as medical advice. Researchers should consult appropriate medical and scientific literature for comprehensive information.
SAFETY PRECAUTIONS: Proper safety equipment, training, and protocols must be employed when handling this product. Follow all institutional biosafety guidelines and regulations.
STORAGE AND DISPOSAL: Store according to specifications. Dispose of unused product and materials according to institutional and regulatory guidelines for biological materials.
By purchasing HCG 5000IU, you acknowledge that you have read, understood, and agree to comply with these terms and restrictions.
| Weight | 0.1 lbs |
|---|---|
| Dimensions | N/A |
Only logged in customers who have purchased this product may leave a review.
support@prymalab.net info@prymalab.net
30 Day return window. Satisfaction guaranteed or your money back.
All orders over %150 in value will receive free shipping.






Reviews
There are no reviews yet.